Key takeaways:
~ Lipoprotein(a) – Lp(a) – is a cholesterol carrier.
~ High Lp(a) levels are strongly linked to an increased risk of heart attacks and aortic stenosis.
~ Genetic variants in the LPA gene drive Lpa(a) levels. It is highly genetic.
~ Knowledge is power here: If you likely have genetically higher Lp(a), you can know to talk with your doctor and get your Lp(a) levels tested.
What is lipoprotein(a)?
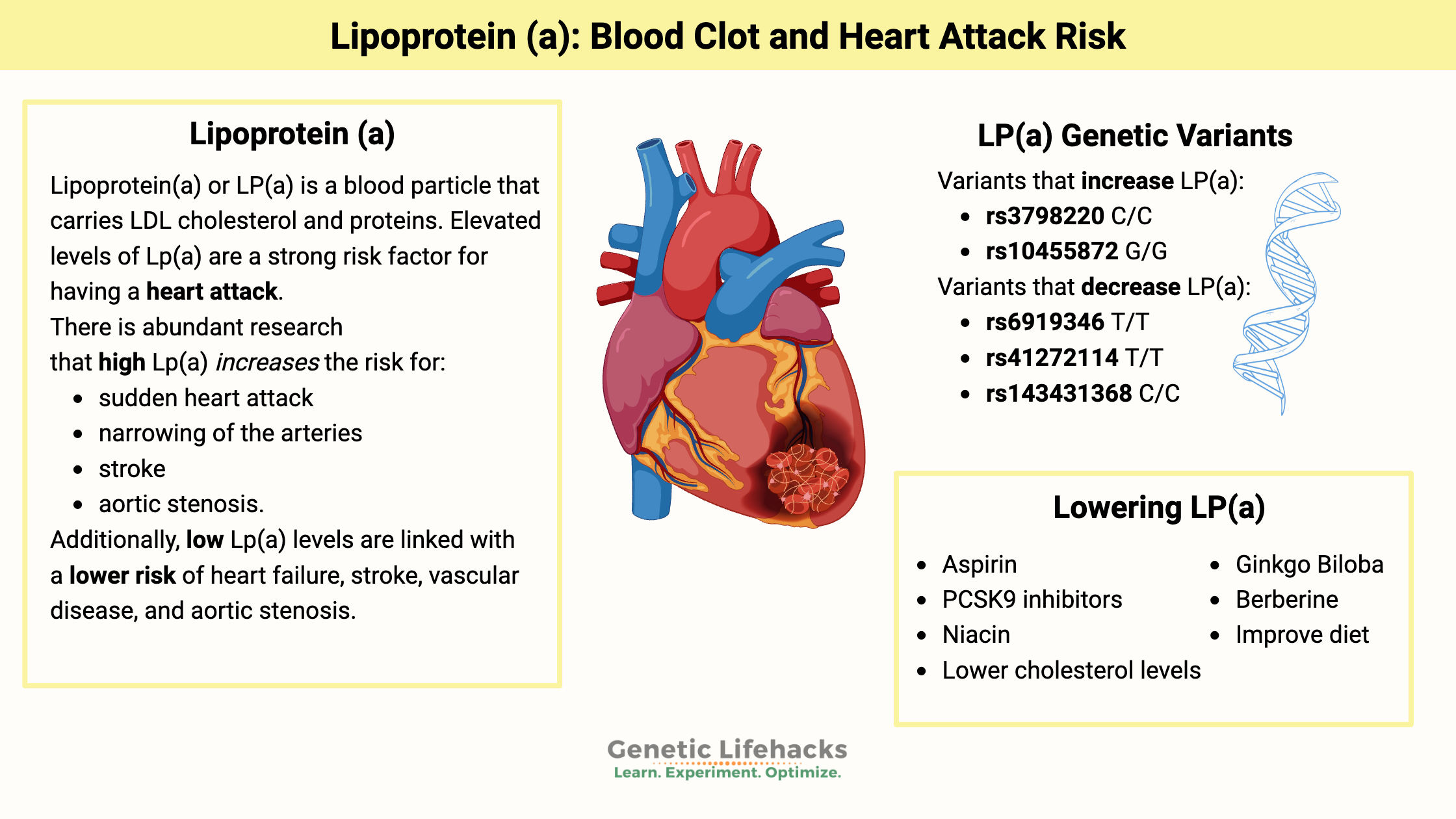
Lipoprotein(a), or Lp(a), is a blood particle that carries LDL cholesterol and proteins. Elevated levels of Lp(a) are a strong risk factor for having a heart attack due to atherosclerotic plaque buildup.[ref]
Lipoproteins are fat-protein packages that transport cholesterol through the bloodstream, including LDL, HDL, and lipoprotein(a).
Atherosclerosis:
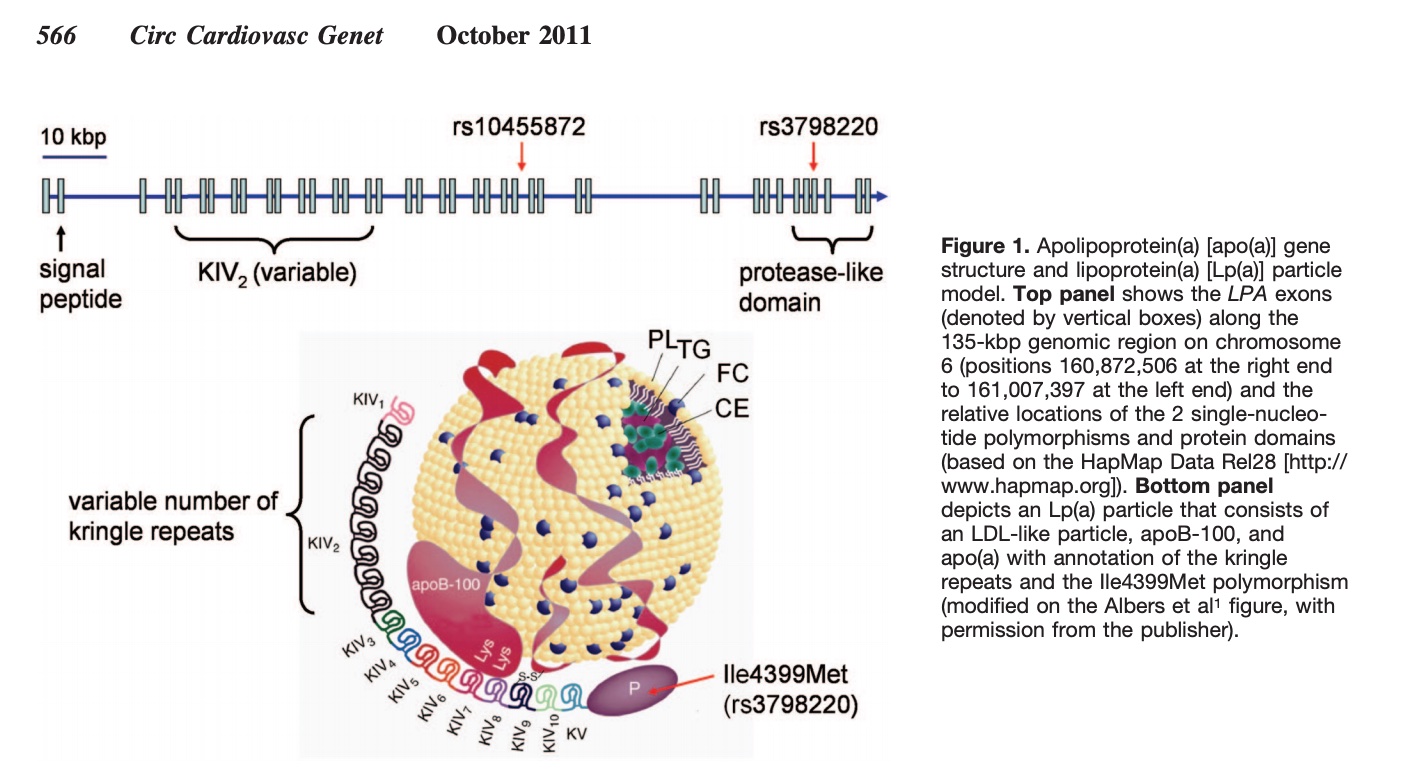
Lipoprotein(a) consists of an LDL particle bound to apolipoprotein(a) [apo(a)] and apoB100. The apo(a) component increases atherosclerosis and promotes clotting by interfering with the body’s clot-dissolving mechanisms. LDL oxidizes within vessel walls, which triggers inflammation. This creates a double-whammy: increased atherosclerotic plaque formation and elevated blood clot risk.[ref][ref]
Prothrombotic effect:
In addition to increasing atherosclerosis, higher Lp(a) levels also have a prothrombotic – clot-forming – effect during inflammation. Lp(a) can bind to fibrin and defensins that are released by neutrophils during infections or inflammation. [ref]
Lp(a) molecule size:
The Lp(a) molecule can vary a lot in size and have different risk levels. You inherit one variant from each parent, and these size differences affect your risk of heart attacks and strokes.[ref]
Lipoprotein(a) levels are hereditary:
“Family history” is always mentioned by the doctor as an important indicator of your risk of heart disease, especially if a family member had a heart attack at a young age. Lp(a) is often the reason that this question is asked.
A significant way that researchers have found family history plays a role in early heart attacks is by the genetic variants that increase lipoprotein(a).
Lp(a) levels are estimated to be 90% hereditary.[ref] (That’s really high when it comes to hereditary estimates!)
High Lp(a) increases the risk of cardiovascular events:
There is abundant research that high Lp(a) significantly increases the risk for:[ref][ref][ref][ref][ref][ref]
- sudden heart attack
- narrowing of the arteries
- stroke
- aortic stenosis
- peripheral artery disease
- heart failure
For example, moderate to high levels of Lp(a) increase the risk of coronary stenosis (narrowing of the arteries) by 67%.[ref]
Additionally, the opposite is true –> low Lp(a) levels are linked with a lower risk of heart failure, stroke, vascular disease, and aortic stenosis.[ref]
A 2024 study showed that high Lp(a) levels increase the risk of heart attacks more than standard modifiable risk factors (SMuRFs), which include diabetes, dyslipidemia, hypertension, and smoking.

The kicker: Shorter lifespan
Genetic studies show that variants linked to high Lp(a) correlate with a shorter lifespan. When averaging together information from more than 100,000 people, the presence of an Lp(a) genetic variant caused an average decrease in lifespan of 1.5 years.[ref]
What is a high level of Lp(a)?
When you get your Lp(a) test results, how do you know if it is just slightly high or seriously scary?
Some researchers consider normal to be less than 50 mg/dl.[ref][ref] Another source says normal Lp(a) levels are less than 30 mg/dl (or 75 nmol/L).[ref]
Risk increases with Lp(a) levels:
A study involving over 58,000 individuals in Denmark showed that major cardiovascular event rates (e.g. heart attacks) increased as Lp(a) levels increased. Lp(a) levels less than 10 mg/dL (18 nmol/L) had the lowest risk.[ref]
- 28% increased relative risk of major cardiac event with Lp(a) 10 to 49 mg/dL (18 – 105 nmol/L)
- 44% increased relative risk of major cardiac event with Lp(a) between 50 to 99 mg/dL (105–213 nmol/L)
- 114% increased relative risk of major cardiac event with Lp(a) ≥100 mg/dL (214 nmol/L)
A 2026 study involving almost 30,000 women showed that the risk of major cardiac events increased almost linearly starting at Lp(a) levels over 30 mg/dL. Most of this risk was attributed to the rs3798220 variant (below in the genotype report section).[ref]
For aortic valve stenosis, there is a 3-fold increase in relative risk for those with Lp(a) levels greater than 90 mg/dl.[ref]
Higher Lp(a) expression is a risk factor for calcific aortic valve disease. [ref]
A recent study in India showed that Lp(a) levels >50mg/dl (105 nmol/L) increased the risk of coronary artery disease in younger people by 2 to 3-fold.[ref]
Not all studies agree: Gender and lipid level interactions
An epidemiological study involving women found that Lp(a) levels were only important in cardiovascular disease if the women also had high cholesterol (>220 mg/dl).[ref]
A 2012 study in people with diabetes found that higher Lp(a) levels did not correlate with an increased risk of heart disease. There was no additional risk above and beyond the high risk from diabetes.[ref]
One problem with the epidemiological studies on Lp(a) is that most of them only last for 5 to 10 years, which may not be enough time to really determine causality. The JAMA study published in January of 2026 was a 30-year study in women; it showed that risk rises with long-term high Lp(a).[ref]
Inflammation as a modifying factor:
A study looking at hsCRP levels along with Lp(a) levels showed that inflammation may be a modifying factor in increasing the risk of cardiovascular disease with Lp(a) levels between 50-100 mg/dL. In individuals with hsCRP <2mg/L, there was no statistically significant cardiovascular disease risk observed. However, with hsCRP ≥2 mg/L, a significant CVD risk was seen at >50mg/dL and even more so at >100mg/dL of Lp(a).[ref]
Lipoprotein (a) Genotype Report
LPA gene: encodes lipoprotein(a). These first two genetic variants cover about 40% of the variation in Lp(a) levels — other, less common variants also raise Lp(a) levels.
Access this content:
An active subscription is required to access this content.
Lifehacks: Reducing high lipoprotein(a)
So what do you do if you carry the risk alleles for high Lp(a)? First, let’s look at testing options, and then I’ll explain multiple research-backed ways of lowering Lp(a) either with diet, natural supplements, or medications.
Knowledge is power here! You aren’t doomed to have a heart attack from your high Lp(a) levels, but you may need to take some action.
Test your Lp(a) levels:
Talk to your doctor or do it yourself:
The only way to know your current Lp(a) level is to get it tested. It may be covered by insurance in your annual well-check, especially if you have a family history of early heart attacks.
You can also get a test done for Lp(a) in the US without going through your doctor. For example, on UltaLabTests, the Lp(a) test currently costs $29. There are other places online to order the Lp(a) test, and there’s also a new, at-home Lp(a) test for $99. (I haven’t used it, so check for reviews on it).
Increased Risk with high CRP:
One study showed that hsCRP >2 mg/L combined with Lp(a) in increasing risk of cardiovascular disease.[ref] hsCRP is also a readily available and inexpensive test. Again, talk with your doctor or get the test done yourself so that you have a baseline to know if the interventions are working for you.
Now let’s take a look at ways you can lower your Lp(a) levels. Keep in mind that you can stack multiple interventions together – consider a dietary change plus supplements, along with talking to your doctor about aspirin therapy or other medications.
Access this content:
An active subscription is required to access this content.
Related Articles and Topics:
PCSK9 Gene: Understanding the variants that cause high or low LDL cholesterol
References:
Arsenault, Benoit J., et al. “Association of Long-Term Exposure to Elevated Lipoprotein(a) Levels With Parental Life Span, Chronic Disease–Free Survival, and Mortality Risk.” JAMA Network Open, vol. 3, no. 2, Feb. 2020, p. e200129. PubMed Central, https://doi.org/10.1001/jamanetworkopen.2020.0129.
Brix, Gitte Stokvad, et al. “Elevated lipoprotein (a) is independently associated with the presence of significant coronary stenosis in de-novo patients with stable chest pain.” American Heart Journal (2025).
Chang, Xinxia, et al. “Lipid Profiling of the Therapeutic Effects of Berberine in Patients with Nonalcoholic Fatty Liver Disease.” Journal of Translational Medicine, vol. 14, Sept. 2016, p. 266. PubMed Central, https://doi.org/10.1186/s12967-016-0982-x.
Chapman, M. John, et al. “Niacin and Fibrates in Atherogenic Dyslipidemia: Pharmacotherapy to Reduce Cardiovascular Risk.” Pharmacology & Therapeutics, vol. 126, no. 3, June 2010, pp. 314–45. PubMed, https://doi.org/10.1016/j.pharmthera.2010.01.008.
Chasman, Daniel I., et al. “Polymorphism in the Apolipoprotein(a) Gene, Plasma Lipoprotein(a), Cardiovascular Disease, and Low-Dose Aspirin Therapy.” Atherosclerosis, vol. 203, no. 2, Apr. 2009, pp. 371–76. PubMed, https://doi.org/10.1016/j.atherosclerosis.2008.07.019.
Chen, Hao Yu, et al. “Association of LPA Variants With Aortic Stenosis: A Large-Scale Study Using Diagnostic and Procedural Codes From Electronic Health Records.” JAMA Cardiology, vol. 3, no. 1, Jan. 2018, pp. 18–23. PubMed, https://doi.org/10.1001/jamacardio.2017.4266.
Chmielewski, K. “[Clinical and bacteriological observations on the use of immediate prostheses made of quickly polymerizing methyl polymetacrylane].” Czasopismo stomatologiczne, vol. 19, no. 5, May 1966, pp. 549–53.
Clarke, Robert, et al. “Genetic Variants Associated with Lp(a) Lipoprotein Level and Coronary Disease.” New England Journal of Medicine, vol. 361, no. 26, Dec. 2009, pp. 2518–28. Taylor and Francis+NEJM, https://doi.org/10.1056/NEJMoa0902604.
Emdin, Connor A., et al. “Phenotypic Characterization of Genetically Lowered Human Lipoprotein(a) Levels.” Journal of the American College of Cardiology, vol. 68, no. 25, Dec. 2016, pp. 2761–72. ScienceDirect, https://doi.org/10.1016/j.jacc.2016.10.033.
Enas, Enas A., et al. “Lipoprotein(a): An Independent, Genetic, and Causal Factor for Cardiovascular Disease and Acute Myocardial Infarction.” Indian Heart Journal, vol. 71, no. 2, Mar. 2019, pp. 99–112. ScienceDirect, https://doi.org/10.1016/j.ihj.2019.03.004.
Erhart, Gertraud, et al. “Genetic Factors Explain a Major Fraction of the 50% Lower Lipoprotein(a) Concentrations in Finns.” Arteriosclerosis, Thrombosis, and Vascular Biology, vol. 38, no. 5, May 2018, pp. 1230–41. ahajournals.org (Atypon), https://doi.org/10.1161/ATVBAHA.118.310865.
Franchini, Massimo, et al. “Lipoprotein Apheresis for the Treatment of Elevated Circulating Levels of Lipoprotein(a): A Critical Literature Review.” Blood Transfusion, vol. 14, no. 5, Sept. 2016, pp. 413–18. PubMed Central, https://doi.org/10.2450/2015.0163-15.
Hanssen, Ruth, and Ioanna Gouni-Berthold. “Lipoprotein(a) Management: Pharmacological and Apheretic Treatment.” Current Medicinal Chemistry, vol. 24, no. 10, 2017, pp. 957–68. PubMed, https://doi.org/10.2174/0929867324666170112110928.
Joshi, Parag H., et al. “Do We Know When and How to Lower Lipoprotein(a)?” Current Treatment Options in Cardiovascular Medicine, vol. 12, no. 4, Aug. 2010, pp. 396–407. PubMed, https://doi.org/10.1007/s11936-010-0077-6.
Kamstrup, Pia R., et al. “Elevated Lipoprotein(a) and Risk of Aortic Valve Stenosis in the General Population.” Journal of the American College of Cardiology, vol. 63, no. 5, Feb. 2014, pp. 470–77. PubMed, https://doi.org/10.1016/j.jacc.2013.09.038.
Kronenberg, F., and G. Utermann. “Lipoprotein(a): Resurrected by Genetics.” Journal of Internal Medicine, vol. 273, no. 1, Jan. 2013, pp. 6–30. DOI.org (Crossref), https://doi.org/10.1111/j.1365-2796.2012.02592.x.
Kronenberg, Florian. “Prediction of Cardiovascular Risk by Lp(a) Concentrations or Genetic Variants within the LPA Gene Region.” Clinical Research in Cardiology Supplements, vol. 14, no. 1, Apr. 2019, pp. 5–12. Springer Link, https://doi.org/10.1007/s11789-019-00093-5.
Laschkolnig, Anja, et al. “Lipoprotein (a) Concentrations, Apolipoprotein (a) Phenotypes, and Peripheral Arterial Disease in Three Independent Cohorts.” Cardiovascular Research, vol. 103, no. 1, July 2014, pp. 28–36. PubMed, https://doi.org/10.1093/cvr/cvu107.
Li, Yonghong, et al. “Genetic Variants in the Apolipoprotein(a) Gene and Coronary Heart Disease.” Circulation: Cardiovascular Genetics, vol. 4, no. 5, Oct. 2011, pp. 565–73. DOI.org (Crossref), https://doi.org/10.1161/CIRCGENETICS.111.959601.
Najjar, Rami S., et al. “Consumption of a Defined, Plant‐based Diet Reduces Lipoprotein(a), Inflammation, and Other Atherogenic Lipoproteins and Particles within 4 Weeks.” Clinical Cardiology, vol. 41, no. 8, Aug. 2018, pp. 1062–68. PubMed Central, https://doi.org/10.1002/clc.23027.
PhD, Chris Masterjohn. “026: The 5 Best Ways to Lower Cholesterol Naturally.” Harnessing the Power of Nutrients, 9 May 2017, https://chrismasterjohnphd.substack.com/p/026-the-5-best-ways-to-lower-cholesterol.
Qi, Qibin, et al. “Genetic Variants, Plasma Lipoprotein(a) Levels, and Risk of Cardiovascular Morbidity and Mortality among Two Prospective Cohorts of Type 2 Diabetes.” European Heart Journal, vol. 33, no. 3, Feb. 2012, pp. 325–34. PubMed, https://doi.org/10.1093/eurheartj/ehr350.
Risch, S. C., et al. “Multiendocrine Assessment in the Dexamethasone Suppression Test.” Psychopharmacology Bulletin, vol. 22, no. 3, Jan. 1986, pp. 913–16.
Rodríguez, M., et al. “Reduction of Atherosclerotic Nanoplaque Formation and Size by Ginkgo Biloba (EGb 761) in Cardiovascular High-Risk Patients.” Atherosclerosis, vol. 192, no. 2, June 2007, pp. 438–44. PubMed, https://doi.org/10.1016/j.atherosclerosis.2007.02.021.
Ronald, James, et al. “Genetic Variation in LPAL2 , LPA , and PLG Predicts Plasma Lipoprotein(a) Level and Carotid Artery Disease Risk.” Stroke, vol. 42, no. 1, Jan. 2011, pp. 2–9. DOI.org (Crossref), https://doi.org/10.1161/STROKEAHA.110.591230.
Song, Zi-Kai, et al. “LPA Gene Polymorphisms and Gene Expression Associated with Coronary Artery Disease.” BioMed Research International, vol. 2017, 2017, p. 4138376. PubMed, https://doi.org/10.1155/2017/4138376.
Viney, Nicholas J., et al. “Antisense Oligonucleotides Targeting Apolipoprotein(a) in People with Raised Lipoprotein(a): Two Randomised, Double-Blind, Placebo-Controlled, Dose-Ranging Trials.” Lancet (London, England), vol. 388, no. 10057, Nov. 2016, pp. 2239–53. PubMed, https://doi.org/10.1016/S0140-6736(16)31009-1.
Vogt, Anja. “Lipoprotein(a)-Apheresis in the Light of New Drug Developments.” Atherosclerosis. Supplements, vol. 30, Nov. 2017, pp. 38–43. PubMed, https://doi.org/10.1016/j.atherosclerosissup.2017.05.025.
Wang, Hui, et al. “Berberine Modulates LPA Function to Inhibit the Proliferation and Inflammation of FLS-RA via P38/ERK MAPK Pathway Mediated by LPA1.” Evidence-Based Complementary and Alternative Medicine, vol. 2019, Nov. 2019, p. e2580207. www.hindawi.com, https://doi.org/10.1155/2019/2580207.
“Why Would My Doctor Order a Lipoprotein(a) Blood Test?” Cleveland Clinic, 11 Dec. 2019, https://health.clevelandclinic.org/why-would-my-doctor-order-a-lipoproteina-blood-test/.