Key takeaways:
- Many common prescription medications can lower specific vitamins and minerals over time.
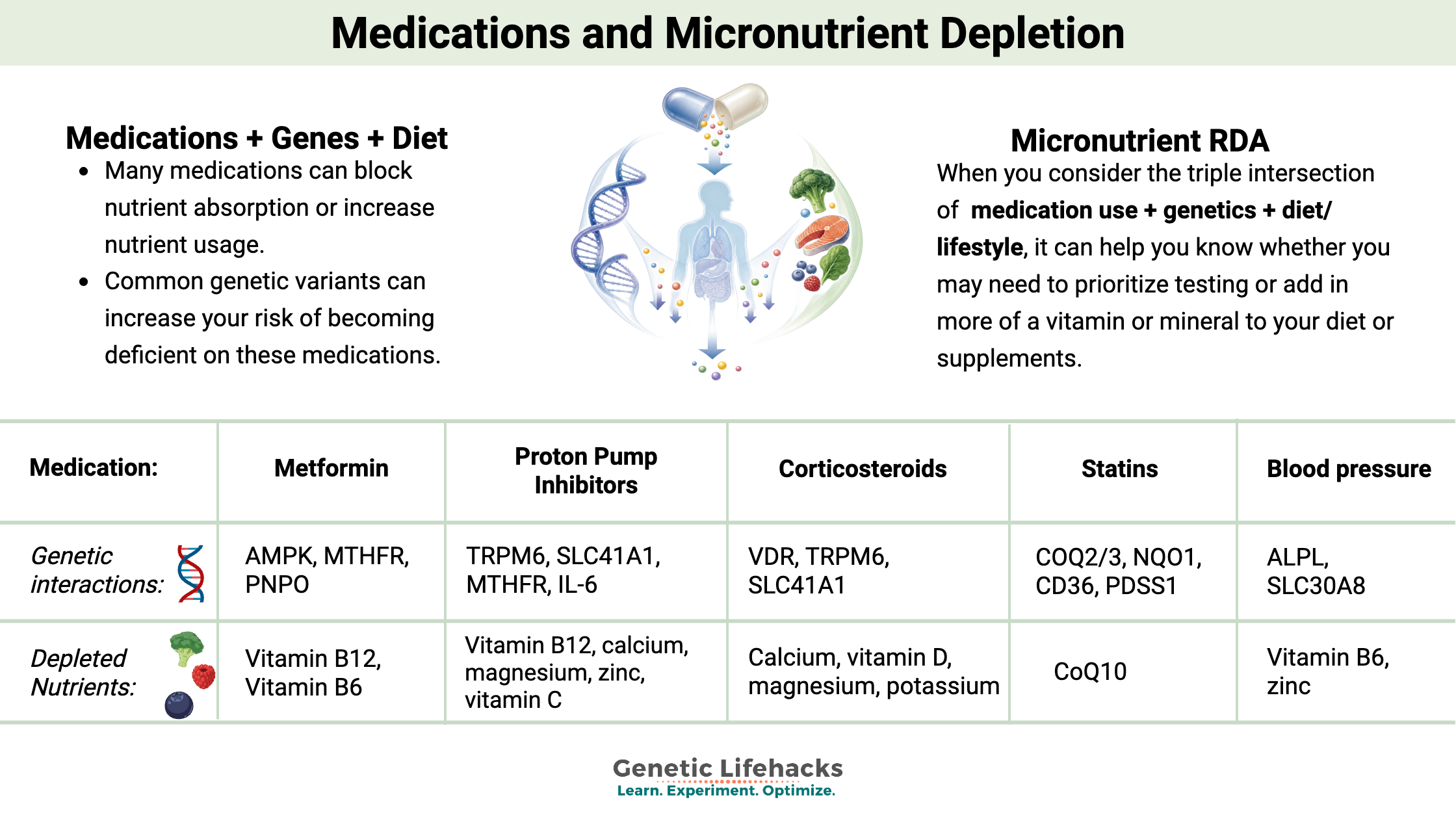
- Genetic variants can increase your risk of becoming deficient while taking certain drugs.
- Combining your medication list, genotype information, and diet helps you decide which micronutrients to test or prioritize in foods/supplements.
- Always talk with your prescribing physician before changing supplements, since nutrients like potassium or vitamin K can alter how medications work.
Medications can decrease vitamin and nutrient levels
In the US, about two-thirds of adults regularly take at least one prescription medication, with many taking multiple drugs.[ref] These drugs can be lifesaving for blood pressure, reflux, diabetes, mood, and more. But some medications often come with a side effect of quietly draining vitamins and minerals over the months or years of use.
Certain medications can block the absorption of micronutrients in the gut or can increase the depletion of specific vitamins or minerals.[ref] At the same time, common genetic variants can also increase your susceptibility to being low in nutrients like B12, folate, magnesium, or vitamin D, and diet and lifestyle can push you further in either direction.
When you look at medication use + genetics + diet/lifestyle together, it can help you identify where you’re most likely to run low and which micronutrients are worth testing or prioritizing in your diet or supplements.
Researchers sometimes call this “drug-induced nutrient depletion” or “drug–nutrient interactions,” and it can show up as fatigue, neuropathy, bone loss, or mood changes that don’t have an obvious cause. Mild deficiencies from medication use may go unnoticed at first, but over time, they can reduce your resiliency. Lower baseline levels of a nutrient can make the effects show up sooner or be more severe. For example, metformin commonly lowers vitamin B12, and people with certain B12-related variants are more likely to develop neuropathy or anemia unless the deficiency is caught and corrected.
How can you use this information?
Below, you’ll see medications along with studies showing which micronutrients may be affected. Logged-in members also see their genotypes for variants that influence the levels of those specific vitamins or minerals.
- Look at the medications you’re taking and nutrients affected
- Check your genetic variants related to that nutrient (Read the full article on the nutrient for more details)
- Consider how long you’ve been on the medication, your typical diet, and any supplements you already use.
- Based on your risk, decide if you should talk to your doctor, test your nutrient level, and/or add foods or supplements to restore your nutrient levels.
Caution: Do not start or stop any supplement without discussing it with your prescribing physician, especially for nutrients like potassium (with ARBs) or vitamin K (with warfarin), which directly affect how these drugs work. This article is for informational and educational purposes only and is not medical advice. Ask your doctor whether lab testing for the specific nutrient is appropriate before making changes.
Use the links below to jump to your medication:
Metformin | PPIs | Statins | Oral Contraceptives | Corticosteroids | Blood Pressure | Beta-Blockers | Diuretics | Aspirin & Acetaminophen | Antibiotics | Antispychotics | Warfarin | Antidepressants
Metformin:
Metformin is a commonly prescribed medication for diabetes or PCOS. It works by affecting the mitochondria and activating an enzyme called AMPK.
Depleted nutrients: Vitamin B12 and Vitamin B6
Vitamin B12: A meta-analysis of 17 studies showed that within 6 weeks to 3 months of use, there is an increased risk of low vitamin B12 in patients who are using metformin. The length of time on the drug also matters. A placebo-controlled trial showed that after 5 years, twice as many patients on metformin (19%) met the definition of low or borderline low B12 (> 298 pg/mL) compared to patients on a placebo.[ref][ref]
Access this content:
An active subscription is required to access this content.
RDAs for Vitamins and Minerals:
Here’s a handy reference for the RDA and Upper daily limit (UL) for the vitamins and minerals covered in this article. Note that taking more than the upper daily limit on some vitamins and minerals can have negative effects, such as long-term high intake of zinc blocking copper absorption.
| Nutrient | Adult RDA / AI | Upper daily limit (UL) |
|---|---|---|
| Vitamin B12 | 2.4 mcg/day | No UL established |
| Folate | 400 mcg/day DFE | 1,000 mcg/day |
| Vitamin B6 | 1.3 mg/day (ages 19–50); 1.7 mg/day (men 51+; women 51+) | 100 mg/day |
| Vitamin C | 75 mg/day (women); 90 mg/day (men) | 2,000 mg/day |
| Vitamin D | 15 mcg/day (600 IU) ages 19–70; 20 mcg/day (800 IU) age 71+ | 100 mcg/day (4,000 IU) |
| Vitamin K | 90 mcg/day (women); 120 mcg/day (men) | No UL established |
| Magnesium | 310–320 mg/day (women); 400–420 mg/day (men) | 350 mg/day from supplements/fortified foods only |
| Zinc | 8 mg/day (women); 11 mg/day (men) | 40 mg/day |
| Selenium | 55 mcg/day | 400 mcg/day |
Related Articles and Topics:
References: