Key takeaways:
- Norepinephrine is both a neurotransmitter that helps with focus, attention, and motivation, and a hormone that affects blood pressure, heart rate, and stress response.
- In the brain, most norepinephrine is produced in the locus coeruleus. It activatesα1, α2, and β adrenergic receptors to fine-tune neurological pathways.
- Norepinephrine is synthesized from dopamine by DBH, cleared from the synapse primarily via the norepinephrine transporter (NET/SLC6A2), and then metabolized by MAO‑A and COMT.
- Genetic variants can shift the baseline levels of norepinephrine and the response to drugs.
- Altered norepinephrine signaling is implicated in ADHD, Alzheimer’s, ME/CFS, Parkinson’s, long Covid, POTS, and mood disorders.
What is norepinephrine (noradrenaline)?
Norepinephrine, also known as noradrenaline, plays two roles in the body – it is both a neurotransmitter and a hormone.
Norepinephrine acts as a neurotransmitter in the brain, involved in alertness, learning, vigilance, and task engagement. It is part of being awake, alert, and focused.[ref]
Norepinephrine can also act as a stress hormone released by the adrenal glands into the bloodstream, where it increases blood pressure and heart rate. Higher norepinephrine levels also slow non-essential functions, like digestion, in response to stress. It is part of the fight or flight response.[ref]
In the brain, norepinephrine has both excitatory and inhibitory effects. It’s generally excitatory when binding to α1– and β-adrenergic receptors, but has inhibitory effects through α2 -adrenergic receptors.[ref]
Terminology: Norepinephrine is the term usually used in the US and in many research studies, but in the UK and other parts of the world, noradrenaline is more commonly used.
Let’s take a look at how norepinephrine is synthesized, which receptors it activates, and how your genes influence norepinephrine levels. We will end with natural ways to balance your norepinephrine levels.
Where is norepinephrine produced in the brain?
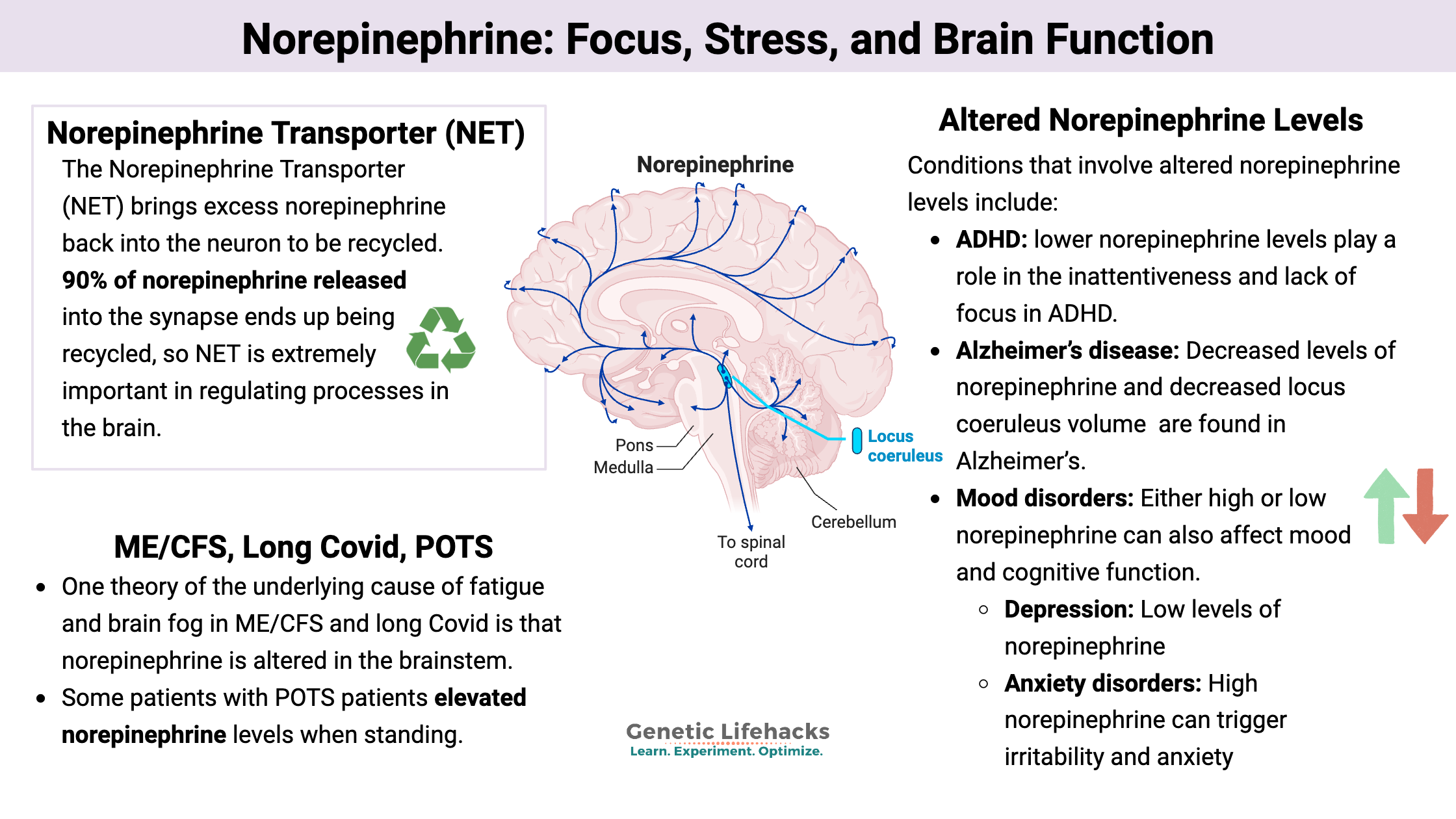
The majority of norepinephrine synthesis in the central nervous system takes place in the locus coeruleus, which is part of the brainstem. The locus coeruleus contains about 30,000 neurons that synthesize the norepinephrine used by the rest of the brain. These neurons project widely into the cortex of the brain, influencing sensory pathways and cognitive functions.[ref]
U-shaped curve: Levels of norepinephrine are tightly controlled, and the different receptors (α1, α2, and β adrenergic receptors) modulate the activity of glutamatergic and GABAergic neurons. Because the receptors are activated at different levels, researchers believe that low norepinephrine, which dominantly activates α2, can over‑inhibit circuits. At intermediate levels, a balanced α2/α1/β activation will optimize the sensory responses and behavior. On the other hand, very high norepinephrine will cause both excessive inhibition or noisy excitation, depending on the type of neuron.[ref]
How is norepinephrine synthesized?
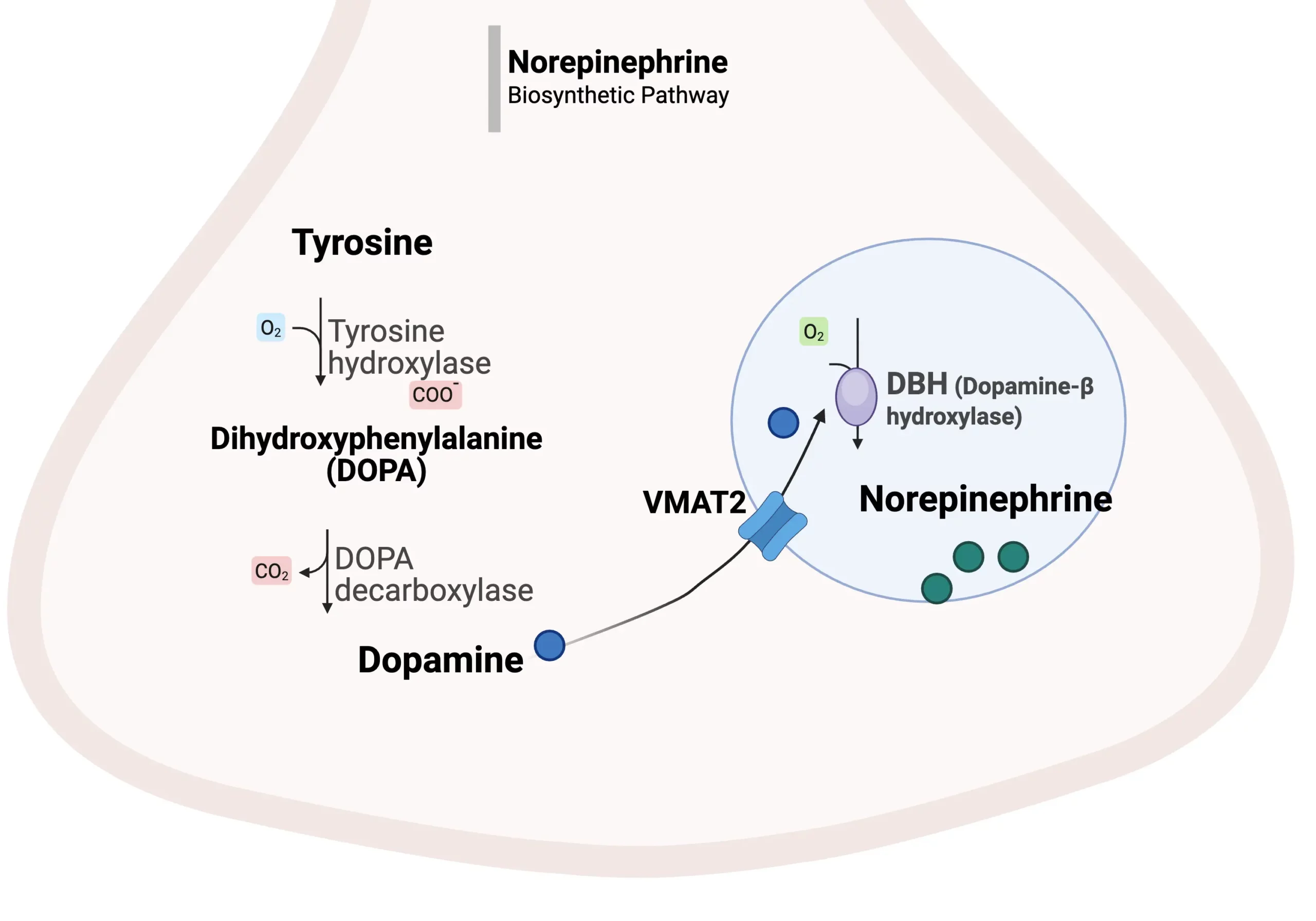
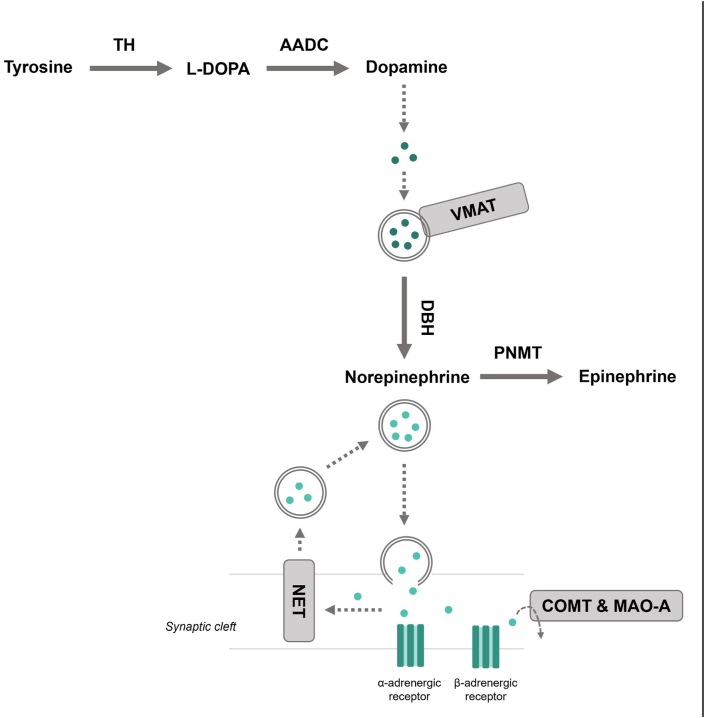
The synthesis of norepinephrine in neurons starts with dopamine, which is packaged into vesicles. An enzyme called dopamine beta-hydroxylase (DBH) converts dopamine to norepinephrine, which is then released into the synapse via the vesicles. [ref]
Backing up on this pathway, dopamine is synthesized from the amino acid tyrosine with the help of the rate-limiting enzyme tyrosine hydroxylase. So you need sufficient tyrosine (amino acid) and tyrosine hydroxylase (enzyme) to produce dopamine, which then gets packaged into vesicles. In the neurons of the locus coeruleus, specifically, the vesicles contain the dopamine beta-hydroxylase enzyme to convert dopamine to norepinephrine. In other areas of the brain, dopamine is simply released as a neurotransmitter and not converted to norepinephrine.
To move dopamine into the synaptic vesicles, neurons use the VMAT2 transporter. Variants in VMAT2 affect mood, addiction, and Parkinson’s risk. It is referred to as the “God gene” due to early studies linking it to spirituality. (Related article: VMAT2 genetic variants)
Once released into the synapse, norepinephrine either binds to one of the adrenergic receptors or can be taken back into the releasing neuron (reuptake). Reuptake controls the amount in the synapse, and the recycled norepinephrine can either be broken down by enzymes (COMT or MAOA) or it can be packaged into vesicles to be released again.[ref]
Related article: MAO-A & MAO-B
Related article: COMT gene variants and neurotransmitter metabolism
Norepinephrine Transporter (NET): Regulating norepinephrine levels in the synapse
Similar to dopamine and serotonin, norepinephrine levels in the synapse are tightly regulated by reuptake into presynaptic neurons.
The Norepinephrine Transporter (NET) brings excess norepinephrine back into the neuron to be recycled and repackaged for release or broken down. Because about 90% of norepinephrine released into the synapse ends up being transported back into the neuron, NET is a major controller of norepinephrine signaling in the brain.[ref]
NET reuptake is a hot target for drug developers. Dysregulation of norepinephrine is thought to play a role in depression, addiction, ADHD, anxiety, personality disorders, PMDD, Parkinson’s, migraines, OCD, and pain disorders. Thus, being able to control norepinephrine levels by manipulating the reuptake is a target of much research.
NET is encoded by the SLC6A2 gene. Interestingly, cocaine is a potent inhibitor of NET, allowing more norepinephrine (and dopamine and serotonin) to stay active in the brain.[ref][ref]
Receptors for norepinephrine:
When released into the synaptic cleft, norepinephrine can bind to and stimulate either alpha- or beta-adrenergic receptors, triggering a signal in the receiving neuron. These G-protein-coupled receptors can have either inhibitory or excitatory effects.
Let’s take a look at each type of receptor.
Alpha-Adrenergic receptors:[ref]
- Alpha-1 receptors are found in smooth muscle and can cause vasoconstriction (narrowing of blood vessels), dilation in the pupil, or contraction of sphincters. Alpha-1 receptors are further subdivided as alpha-1a, alpha-1b, and alpha-1d.
Genes: ADRA1A ADRA1B, and ADRA1D - Alpha-2 adrenergic receptors are primarily presynaptic receptors that are part of an inhibitory feedback loop in the brain to limit the release of excess norepinephrine.
Genes: ADRA2A, ADRA2B, and ADRA2C
Beta-adrenergic receptors:
There are three types of beta-adrenergic receptors:[ref][ref]
- Beta-1 adrenergic receptors are found in various regions of the brain as well as in the peripheral nervous system, where they increase heart rate. The cardioselective beta blockers (e.g., metoprolol) affect beta-1 adrenergic receptors.
Gene: ADRB1 - Beta-2 adrenergic receptors are also found in the brain as well as the peripheral nerves, controlling vasodilation and bronchodilation in the lungs. Non-selective beta blockers (e.g., propranolol) affect both beta-1 and beta-2 adrenergic receptors.
Gene: ADRB2 - Beta-3 adrenergic receptors are found in adipose (fat) tissue, bladder, the retina of the eye, heart, and gallbladder.
Gene: ADRB3
Note that while much of the focus is on the neurological effects of norepinephrine, other cell types in the central nervous system, including microglia, also have adrenergic receptors on their cell surface.[ref]
Norepinephrine vs epinephrine: Norepinephrine (noradrenaline) is structurally similar to epinephrine (adrenaline), which is also released from the adrenal glands in response to stress. They usually work together when released in response to a stressor. Norepinephrine more strongly activates α receptors and β1 receptors, while epinephrine more potently activates β2 receptors, especially in the lungs and blood vessels.
Breaking down norepinephrine
Once taken into a neuron or even after being released into the synaptic cleft, norepinephrine can be broken down by two enzymes: MAO-A or COMT. Both of these enzymes break down catechol neurotransmitters, including norepinephrine, helping to regulate the amount that is active in the brain and in the body.[ref]
Variants in both MAOA and COMT are common and can affect levels of norepinephrine.
Effects of norepinephrine:
The effects of norepinephrine depend on the location and the receptors that it acts on.
Suppresses neuroinflammation: In the brain, norepinephrine acts directly on the brain’s immune cells, called microglia, to suppress the release of proinflammatory cytokines. It also facilitates the clearance of metabolic byproducts through the glymphatic system during deep sleep.[ref]
Balances excitability in the brain: The feedback loops and inhibitory effects of the alpha adrenergic receptors help to fine-tune how neurons fire in the brain — preventing excitotoxicity while at the same time increasing attention.[ref]
Take ADHD as an example: One reason for an inability to focus is not enough norepinephrine – or norepinephrine not being present in the synapse long enough. The ADHD drug atomoxetine (Strattera) is a NET inhibitor, which allows for more norepinephrine to remain in the synapse instead of reuptake via NET.[ref]
Increases inflammatory lipids: On the other hand, when norepinephrine is released as a stress hormone, it can stimulate the production of prostaglandins from arachidonic acid. [ref]
Conditions that involve altered norepinephrine levels:
Research points to altered norepinephrine levels affecting the brain and neurological conditions in multiple ways.
| Condition | Proposed NE pattern | Key mechanism(s) mentioned | Example therapy link |
|---|---|---|---|
| ADHD | Often low or insufficient NE in synapse | Reduced NE tone and altered dopamine signaling in prefrontal cortex | NET inhibitors (atomoxetine) and stimulants prolong catecholamine signaling |
| Depression | Low NE associated with low motivation and fatigue | Combined alterations in NE, dopamine, and serotonin | SNRIs and some adjuncts (e.g., creatine) target NE pathways |
| Anxiety | Often high NE in some circuits | Increased NE associated with irritability and anxiety | Beta blockers, NET/MAO modulation, non‑pharmacologic calming strategies |
| Alzheimer’s | Reduced LC NE | LC degeneration, increased neuroinflammation, cholinergic interplay | Research on NE‑modulating approaches is ongoing |
| Parkinson’s | Lower NE due to LC α‑synuclein | LC involvement in addition to dopaminergic neuron loss | May influence non‑motor symptoms |
| ME/CFS & long COVID | Reduced NE pathway activity in CSF | Energy‑intensive DBH conversion and limited ATP; PEM link | Solriamfetol trial suggests benefit of NE/DA reuptake inhibition |
| POTS (hyperadrenergic) | Elevated NE upon standing | Excess sympathetic outflow; NET inhibition worsens tachycardia | Treatment differs by subtype; some may not tolerate NET blockers |
| Neuropathic pain | Dual roles; NE can dampen or aggravate pain | Descending inhibitory NE pathways via α2, but tissue injury may flip effects | SNRIs and TCAs use NE reuptake inhibition for analgesia |
Let’s dive into each of these in more detail.
ADHD:
Along with alterations in the dopaminergic system, lower norepinephrine levels are thought to play a role in the inattentiveness and lack of focus in ADHD. Dopamine regulation is also affected in ADHD, so the effect on norepinephrine may be downstream of dopamine. Alternatively, some animal models point to negative feedback effects from norepinephrine driving the dopamine dysregulation. Note that many current ADHD medications act on norepinephrine reuptake as well as dopamine.[ref]
Alzheimer’s disease:
One part of the pathology seen in the Alzheimer’s brain is decreased locus coeruleus volume and decreased levels of norepinephrine. The loss of norepinephrine plays a role in the pathology of Alzheimer’s in multiple ways, along with the cholinergic dysfunction. The alpha-2 adrenergic receptors affect the release of acetylcholine, and norepinephrine also affects neuroinflammation by downregulating inflammatory cytokine production in the microglia.[ref]
Parkinson’s disease:
While Parkinson’s primarily involves dopaminergic neuron dysfunction, the accumulation of alpha-synuclein in the locus coeruleus leads to decreased norepinephrine levels, exacerbating symptoms. [ref]
Mood disorders:
Either high or low norepinephrine can also affect mood and cognitive function. It’s a U-shaped curve, with both low levels and chronically elevated levels worsening symptoms, while mid‑range activity tends to be associated with better cognitive performance and emotional balance.[ref]
- Depression: Low levels of norepinephrine are strongly linked to low motivation, fatigue, and lethargy in depressive disorders. In depressive disorders, low norepinephrine combines with altered dopamine and serotonin levels in driving symptoms.[ref]
- Anxiety disorders: High norepinephrine can trigger irritability and anxiety – along with changes to other neurotransmitters. [ref]
Neuropathic pain:
Under normal conditions, the release of norepinephrine dampens pain signals by calming nerve activity (alpha-2 adrenergic receptor activation). When the inhibitory signal from the brainstem down the spinal cord is inhibited or weakened, chronic pain can develop. By blocking the reuptake of norepinephrine, SNRIs and tricyclic antidepressants have an anti-inflammatory effect in the pain neurons.[ref] However, it isn’t as straightforward as norepinephrine always being protective against neuropathic pain. In situations with tissue injury, norepinephrine can aggravate pain.[ref]
Connections to ME/CFS, Long Covid:
One theory of the underlying cause of fatigue and brain fog in ME/CFS and long Covid is that norepinephrine is altered in the brainstem.
Let’s take a look at some of the recent studies on this:
A 2026 study looked at neurotransmitter levels in ME/CFS and long Covid patients. Specifically, they sampled cerebral spinal fluid levels of catecholamine neurotransmitters and their metabolites. The norepinephrine pathway activity was lower than normal, but the dopamine pathway activity was normal. They correlated the lower norepinephrine activity with post-exertional malaise (PEM) severity.[ref]
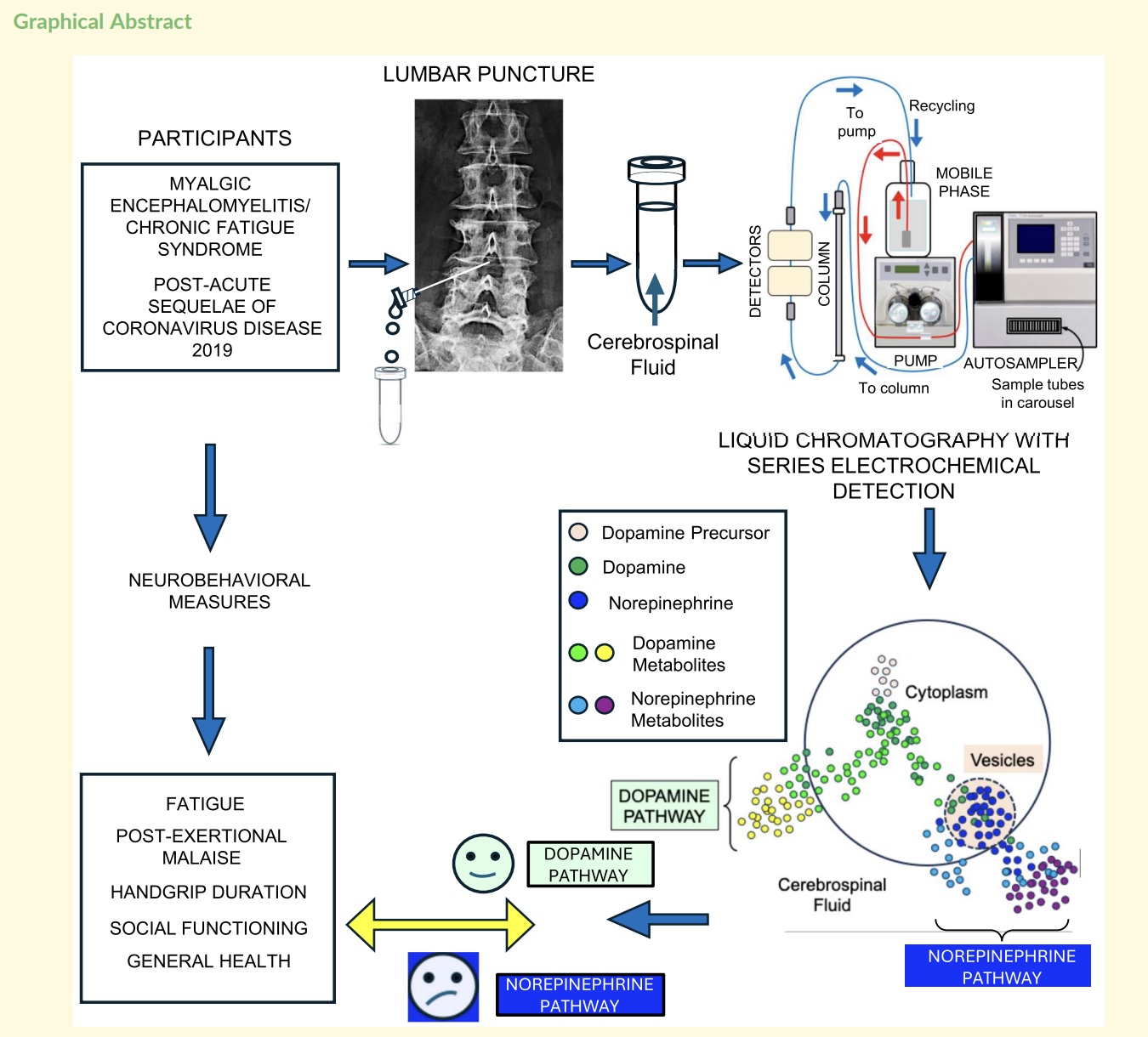
A 2025 double-blind, randomized, placebo-controlled clinical trial looked at the effect of solriamfetol, a norepinephrine and dopamine reuptake inhibitor. The trial results showed improvement in fatigue and cognitive function scores after 8 weeks, compared to placebo.[ref]
Norepinephrine and POTS:
POTS – postural orthostatic tachycardia syndrome – is characterized by a significant increase in heart rate within a few minutes of standing (e.g.,>30 bpm increase). One change noted in patients is that some POTS patients have elevated norepinephrine levels when standing, which some call a hyperadrenergic (excess norepinephrine) subtype of POTS.[ref]
In an effort to understand the role of norepinephrine in POTS, researchers tested a medication that inhibits NET (norepinephrine reuptake transporter), which thereby increases the availability of norepinephrine in the synapse. The results showed worsened symptoms and even more of an increase in heart rate upon standing with higher norepinephrine in the POTS subtype.[ref]
Note that not everyone with POTS is reacting the same way, and not everyone has what some call the hyperadrenergic type of POTS.
Norepinephrine deficiency: DBH mutations
Dopamine beta-hydroxylase, which is encoded by the DBH gene, converts dopamine to norepinephrine.
Rare mutations in the DBH gene can cause dopamine beta-hydroxylase deficiency, which is an autosomal recessive genetic condition affecting the autonomic nervous system. Symptoms usually appear during infancy, but some people aren’t diagnosed until later in childhood or adolescence. Hypotension and ptosis are early signs of the condition, but by adolescence, most with dopamine beta-hydroxylase deficiency will have orthostatic hypotension, or a drop in blood pressure upon standing. The orthostatic hypotension can then cause dizziness, fainting, or problems with exercising.[ref]
Genotype Report: Norepinephrine
Bigger picture: Norepinephrine levels are affected by other pathways prior to synthesis. Upstream of norepinephrine synthesis is dopamine. Please see the full article on dopamine synthesis for variants that affect dopamine levels. Tetrahydrobiopterin (BH4) affects tyrosine conversion. In neurons, dopamine is moved into vesicles where it is converted into norepinephrine.VMAT2 is integral there.
| Step | Key component | Main function | Common gene(s) | Example impact of variants |
|---|---|---|---|---|
| Synthesis from tyrosine | Tyrosine hydroxylase, BH4 | Converts tyrosine to L‑DOPA | TH, GCH1 (BH4) | Rate‑limiting step; variants can reduce dopamine and downstream norepinephrine synthesis |
| Conversion to dopamine | DOPA decarboxylase | Converts L‑DOPA to dopamine | DDC | Alters dopamine availability for norepinephrine synthesis |
| Vesicular loading | VMAT2 | Transports dopamine into vesicles | SLC18A2 (VMAT2) | Affects vesicular dopamine and NE production; linked to mood and addiction |
| Dopamine → norepinephrine | DBH | Converts dopamine to norepinephrine in vesicles | DBH | Lower DBH can shift balance toward higher dopamine and lower norepinephrine |
| Release & reuptake | NET | Clears norepinephrine from synapse | SLC6A2 | Alters norepinephrine persistence and response to NET‑targeting drugs |
| Metabolism | MAO‑A, COMT | Break down norepinephrine | MAOA, COMT | Slow variants can increase catecholamine levels and change supplement responses |
| Receptor signaling | α and β receptors | Mediate excitatory/inhibitory effects | ADRA1/2, ADRB1/2/3 | Influence autonomic tone, pain, mood, and cardiovascular responses |
Synthesis of norepinephrine: DBH
DBH gene: encodes dopamine beta-hydroxylase, a copper-dependent enzyme that catalyzes the conversion of dopamine to norepinephrine. Higher dopamine can increase motivation and drive, but it can also cause restlessness, agitation, difficulties in concentrating, and, at very high levels, paranoia or psychosis.
Access this content:
An active subscription is required to access this content.
Lifehacks: Norepinephrine Solutions
Diet and lifestyle:
Protein-rich foods:
Tyrosine is the amino acid needed for dopamine and norepinephrine synthesis. Food high in tyrosine includes meats, chicken, fish, eggs, cheese, and nuts.
Exercise:
Studies show that aerobic exercise increases dopamine and norepinephrine levels.
Cold exposure:
Intermittent cold exposure, such as a cold plunge, cold shower, or even just cooling the palms and feet, can increase norepinephrine levels.[ref][ref]
Vitamins and Minerals:
Vitamin C and Copper are cofactors for the DBH reaction, converting dopamine to norepinephrine.[ref]
Copper:
Copper deficiency can exacerbate the effect of genetically lower DBH expression. In people on copper-chelator drugs (disulfiram), the combination with low DBH expression increased the risk of paranoia and psychosis when combined with dopamine stimulation (cocaine).[ref][ref] Note that copper is a mineral that is needed in low levels but can be detrimental at higher levels. Testing may be helpful before supplementing with copper. Foods high in copper include organ meats, shellfish, and dark chocolate.
Vitamin C:
Vitamin C (ascorbic acid) is another cofactor that can affect the availability of norepinephrine. In a study of neurological patients, it was found that they had lower than normal DBH levels along with low serum copper and ascorbic acid.[ref]
Supporting brain energy:
The study on ME/CFS and long Covid showed low norepinephrine in the spinal fluid, and explained that the packaging and conversion of dopamine to norepinephrine was an energy-intensive process, with the theory that limited ATP may be decreasing the release of norepinephrine.
Creatine for brain energy: Studies on creatine for sleep deprivation show that supplemental creatine helps to increase norepinephrine levels when the brain is tired. Creatine also helps with depression in women for whom SNRI (serotonin norepinephrine reuptake inhibitors) didn’t work. [ref][ref] Supplemental creatine is also going to help with increasing methyl groups if the methylation cycle is under strain.
d-Ribose:
d-Ribose is a simple sugar available as a supplement that may be beneficial for supporting ATP production in the brain.[ref]
Increasing norepinephrine levels with natural supplements:
Keep in mind that norepinephrine levels can be increased by blocking NET or by increasing the release from vesicles. If the mechanism is known, I’ll include it where relevant.
Access this content:
An active subscription is required to access this content.
Related articles and topics:
Dopamine Synthesis SNPs: Genes, lifestyle, diet, and dopamine optimization
References: