Key takeaways:
- The COMT enzyme is a key factor in the metabolism of neurotransmitters, including those involved in pain sensation.
- Blocking the COMT enzyme causes chronic pain by sensitizing certain pain receptors and increasing inflammatory cytokines.
- Polymorphisms in the COMT gene affect how the enzyme works and how sensitive people are to perceiving pain.
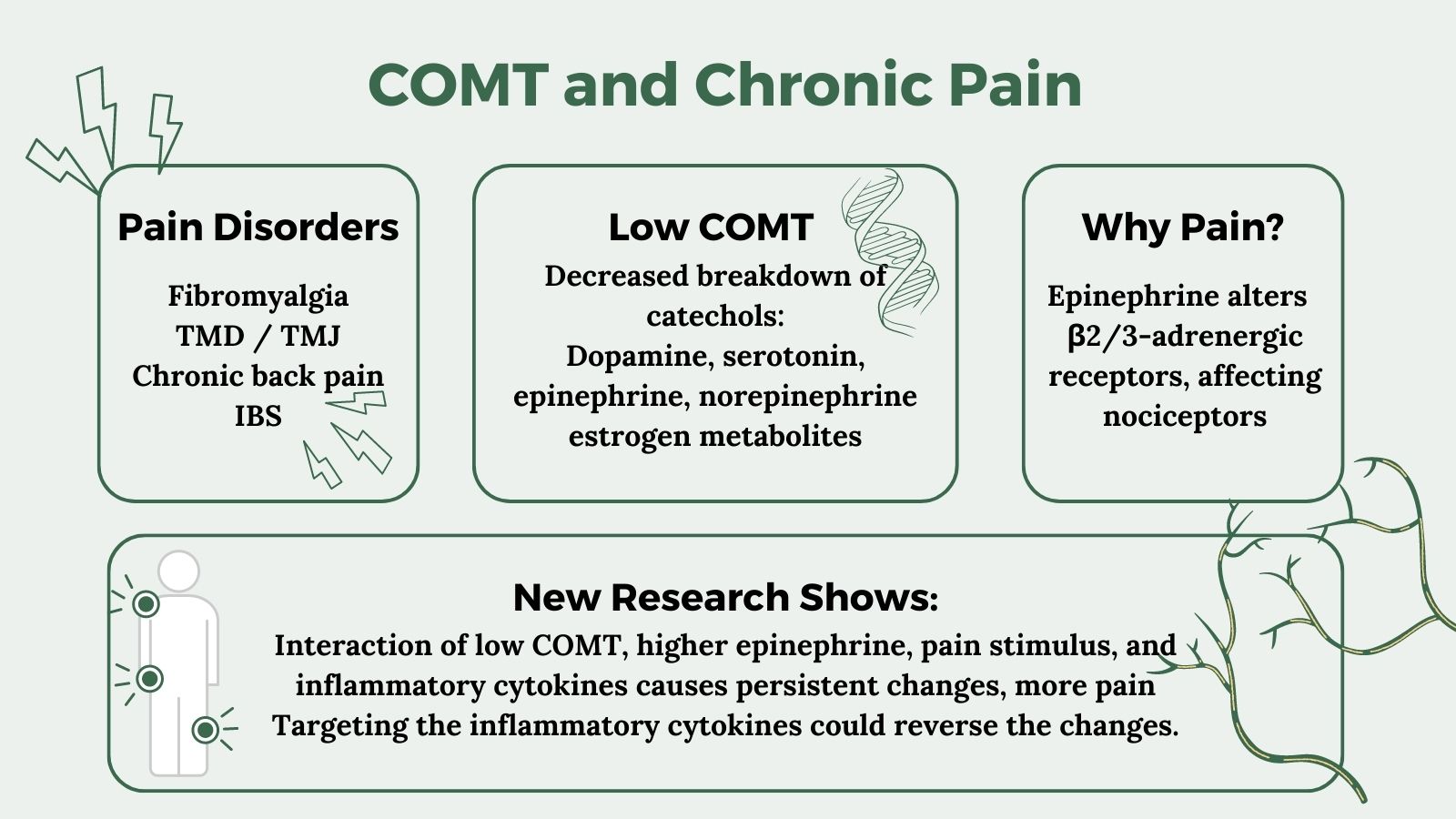
- COMT SNPs affect an individual’s pain levels in chronic pain disorders such as fibromyalgia, TMJ, back pain, and IBS.
<b>Members</b> will see their genotype report below and the solutions in the Lifehacks section. <a href=”https://www.geneticlifehacks.com/membership/”>Consider joining today</a>.
COMT gene and feeling pain:
The COMT gene encodes an enzyme called catechol-O-methyltransferase, which breaks down catechols. Catechols are a class of molecules that includes neurotransmitters such as dopamine, epinephrine, and norepinephrine.
Other catechols include estrogen metabolites, certain drugs, and natural substances with a catechol structure.
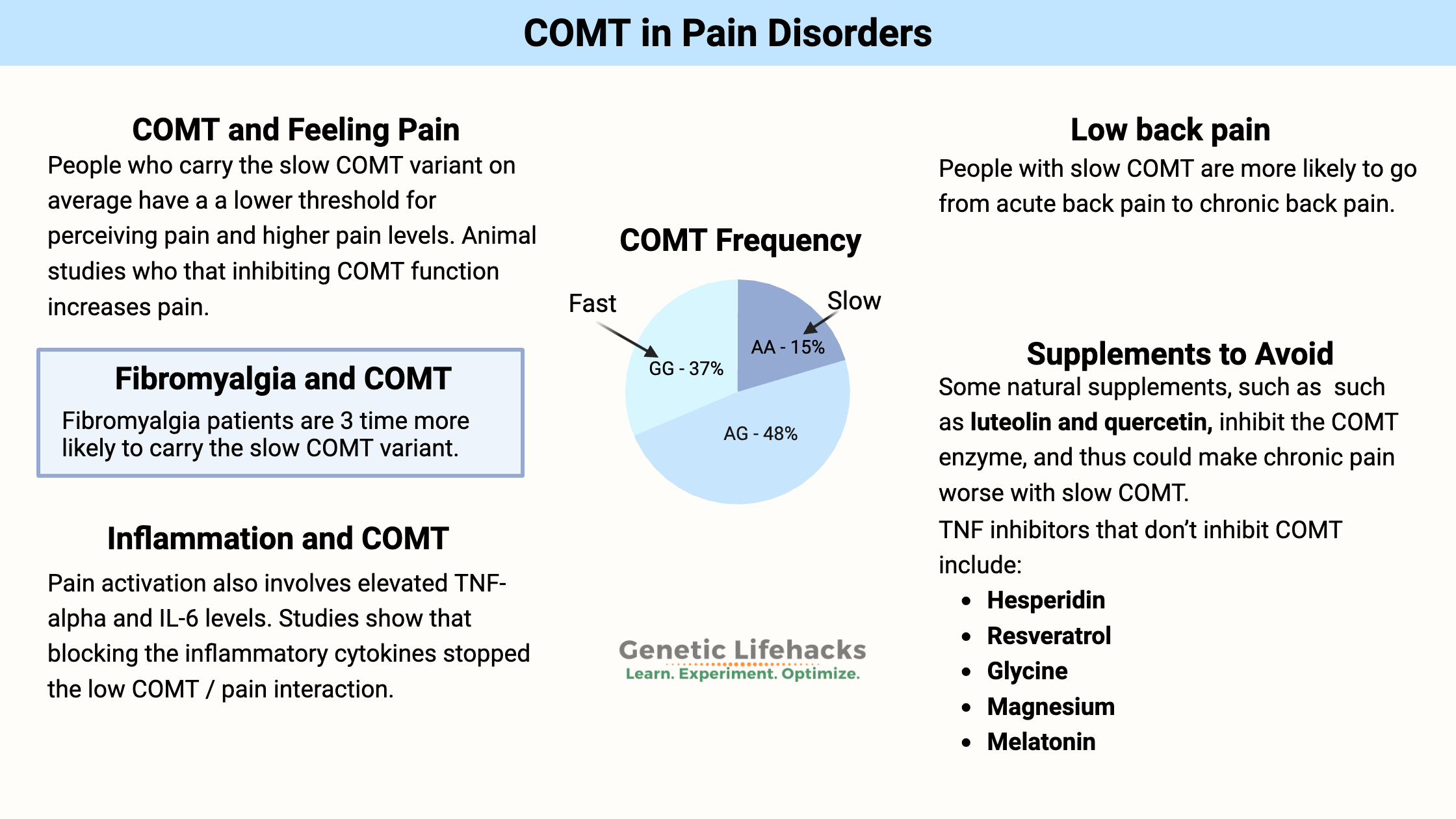
Neurotransmitters are the molecules that nerve cells use to send signals – including telling the brain that you are experiencing pain. Genetic polymorphisms in the COMT gene can affect how much of the enzyme is produced, and thus how likely someone is to experience pain.[ref]
A well-studied variant in the COMT gene is known as Val158Met. The Met/Met genotype is associated with lower COMT activity, and thus slower breakdown of neurotransmitters. In regards to pain disorders, the decreased COMT enzyme alters the level of neurotransmitter available to activate a specific type of adrenergic receptor in peripheral nerves that send pain signals.
People with the Met/Met genotype are likely to have a lower threshold for perceiving pain and higher pain levels.[ref]
Take back pain, for example:
Many people end up dealing with chronic back pain that isn’t due to injury, and disc degeneration is often blamed. The majority of people with disc degeneration don’t actually feel it, but for some, there is chronic and debilitating back pain.[ref] Just to be clear: COMT isn’t the only gene involved in back pain. There are multiple factors, including other inflammation-related genes.Related article: Back Pain and Your Genes
Functional Pain Syndromes (FPS):
Chronic pain conditions such as fibromyalgia, temporomandibular disorders, tension headaches, and irritable bowel syndrome are categorized as “functional pain syndromes”. Researchers tie these disorders to being influenced by the COMT genetic variants.[ref]Let’s take a look at some of the research on how COMT plays a role in pain-related disorders.
Fibromyalgia pain and COMT:
A study involving 112 fibromyalgia patients compared to a matched control group found that they were 3-times more likely to have the slow COMT variant. [ref] Another study found that women with fibromyalgia and the slow COMT variant had more pain than women without the slow variant.[ref]
Is the COMT low-function (slow) variant more common in women with fibromyalgia? It seems that way. A study of over 100 fibromyalgia patients found that they were more likely to carry the slow COMT variant, compared to a healthy control group.[ref]
TMJ, jaw pain, and COMT:
Temporomandibular disorders (TMD) include pain and dysfunction of the temporomandibular joint (TMJ) and jaw pain, especially when chewing.
Pain sensitivity genotyping based on the COMT gene showed that the lower pain sensitivity type cuts the risk of TMJ pain by 2.3-fold.[ref]
Another study looked at the interaction of stress, low COMT activity, and TMD. The study showed that higher stress levels combined with low COMT activity significantly increased the risk of TMD pain.[ref]
Low back pain:
A study of people with low back pain and sciatica found that patients with the slow COMT variant had more back pain and slower recovery.[ref]
One study found that people who tend to go from acute back pain (e.g. threw my back out moving a piano) to chronic lower back pain also were more likely to have higher pain sensitivity throughout the body. This is consistent with other studies that show widespread hypersensitivity to pressure and cold in painful conditions such as TMJ, fibromyalgia, and more. The study also identified COMT and BDNF genetic variants as being important in determining whether acute back pain progresses to chronic lower back pain. [ref]
Not all studies show that COMT causes pain:
Genetic studies don’t always come to the same conclusion. A 2010 study of over 350 people with functional pain disorders found no differences in COMT variants.[ref]
Studies on pain after surgery often do not find that COMT variants make a significant difference.[ref][ref]
Why does low COMT cause more pain with chronic pain syndromes?
There’s a lot of research showing a connection between low COMT genetic variants and pain syndromes. However, the slower breakdown of neurotransmitters doesn’t really explain the ‘why’…
Research into the mechanisms and pathways involved in low COMT and pain shows that the decreased breakdown of epinephrine causes persistent changes in the beta 2 adrenergic receptors which are found on peripheral nerves that sense pain and mechanical stimulation.[ref]
β2 and β3-adrenergic receptors are activated by epinephrine, a catechol neurotransmitter that is broken down by COMT. One place in the body where β2 and β3 -adrenergic receptors are found is in nociceptive pain receptors that react to heat, pressure, cold, or acid. Activation of these receptors can directly cause pain.
A 2007 animal study showed that strong inhibition of COMT with a drug caused increased pain. The researchers found that: “low COMT activity leads to increased pain sensitivity via a β2/3-adrenergic mechanism.”[ref]
This discovery led to further research into how low COMT causes chronic pain via the β2– and β3-adrenergic receptors.
Research shows that pharmacological inhibition of COMT increases the mechanical sensitivity of pain receptors.
In an animal study, blocking COMT with an inhibitor drug for 14 days caused the pain hypersensitivity to persist for at least three weeks after the inhibitor was discontinued.
Two weeks of COMT inhibitor treatment also caused an increase in inflammatory cytokines (TNFα, IL-1β, and IL-6) and activated microglia and astrocytes in the nervous system.
TNF-blocking drugs, such as those used in autoimmune diseases, were able to alleviate the pain. The study concluded: “These results suggest that peripheral β2– and β3ARs drive persistent COMT-dependent functional pain via increased activation of immune cells and production of pro-inflammatory cytokines, which promote neuroinflammation and nociceptor activation. Thus, therapies that resolve neuroinflammation may prove useful in the management of functional pain syndromes.”[ref]
Thus, lower COMT levels combined with inflammation cause persistent pain when specific beta-adrenergic receptors are involved in the sensing of the pain stimulus.
One paper explains that increased adrenergic receptor activation can actually decrease pain in certain situations, but it increases pain in other types of receptors.
- In peripheral pain (muscles, joints) and nociceptive pain, the higher catecholamine neurotransmitter levels increase the pain, especially when inflammation is involved.
- The opposite seems to be true for neuropathic pain (e.g. peripheral neuropathy), where increasing the catecholamine neurotransmitters may help relieve the pain. [ref]
Propranolol response:
Propranolol is a beta-adrenergic receptor antagonist (beta blocker) that is sometimes prescribed for persistent pain.
Researchers have found that propranolol is more effective in reducing facial nerve pain in people with the faster COMT variants than in those with the slow COMT enzyme function.[ref]
For musculoskeletal pain, researchers found that people with intermediate or slow COMT function were more likely to benefit from propranolol for pain relief.[ref]
COMT Genotype Report:
COMT Val158Met:
GGVal/Val – fast (higher) COMT activity higher pain thresholdyour genotypeAGVal/Met – intermediate COMT activity (most common genotype in Caucasians); intermediate pain sensitivityyour genotypeAAMet/Met – slow (40% lower COMT activity) lower pain threshold, higher dopamine; more pain in chronic pain situations more common in fibromyalgia patientsyour genotypeYour genotype for rs4680 is — (not in your raw data).Research & references
GGtypicalyour genotypeGTrisk of higher pain sensitivityyour genotypeTTrisk of higher pain sensitivityyour genotypeYour genotype for rs6267 is — (not in your raw data).Research & references
Lifehacks:
Talk with your doctor or health care professional before starting any supplement or dietary change. Always check with your doctor or pharmacist if you are taking any medications before starting a new supplement. Some of the natural supplements that are TNF-alpha inhibitors can lower blood pressure and may interact with medications.In a nutshell, the catechol-o-methyltransferase – COMT – enzyme transfers a methyl group to a catechol to change the molecule.
A methyl group is simply one carbon plus three hydrogens. It is used in several different cellular reactions to change one molecule into another. For example, serotonin is converted to melatonin in a two-step process, one of which is the addition of a methyl group.
It may seem that a chronic pain condition could be helped by adding more methyl groups through supplements, but this may not be the best plan.
With the low (slow) COMT genetic variant, you may want to be careful and not overload the system with too many methyl groups at one time.
Many people with low COMT function report that supplements such as methylfolate, SAMe, and methylB12, which provide a large dose of methyl donors, can cause mood swings — feeling good shifts to irritability, anger, and anxiety.
The influx of methyl groups can be used by COMT to convert neurotransmitters, estrogens, and other molecules with a catechol structure. Suddenly altering the rate at which neurotransmitters are metabolized may cause mood changes.
Blocking inflammation to stop COMT-driven pain:
Researchers have found that low COMT or drug inhibition of COMT leads to increased pain sensitivity through activation of beta-2 adrenergic receptors.
Recently, a study showed that this pain activation also involves inducing nitric oxide formation and that elevated TNF-alpha and IL-6 are involved. Blocking the inflammatory cytokines stopped the low COMT / pain interaction.
The conclusion of the study: “Additionally, inhibition of NO synthases and neutralization of the innate immunity cytokines TNFα, IL-1β, and IL-6 blocked the development of COMT-dependent pain.”[ref]
Reversing pain takes time:
Another study on pain induced by blocking the COMT enzyme found that the pain persisted for weeks after the COMT enzyme was unblocked. The authors concluded: “This study demonstrates that sustained stimulation of β2– and β3ARs produces functional pain that persists after removal of the causal stimulus…”[ref]In addition, this research study also found that the persistent pain was due to increased TNFα, IL-1β, and IL-6 and microglial activation, and that blocking TNF-alpha was effective in reducing the pain (in animals).[ref]
Natural TNF inhibitors:
Access this content:
An active subscription is required to access this content.
Graphical Overview:
Related articles:
Familial Mediterranean Fever: Mimics fibromyalgia, arthritis, inflammation
References:
Abbas, Amr M., and Hussein F. Sakr. “Effect of Magnesium Sulfate and Thyroxine on Inflammatory Markers in a Rat Model of Hypothyroidism.” Canadian Journal of Physiology and Pharmacology, vol. 94, no. 4, Apr. 2016, pp. 426–32. PubMed, https://doi.org/10.1139/cjpp-2015-0247.Allen, Patricia J. “Creatine Metabolism and Psychiatric Disorders: Does Creatine Supplementation Have Therapeutic Value?” Neuroscience and Biobehavioral Reviews, vol. 36, no. 5, May 2012, pp. 1442–62. PubMed Central, https://doi.org/10.1016/j.neubiorev.2012.03.005.Barbosa, Flávia Regina, et al. “Influence of Catechol-O-Methyltransferase (COMT) Gene Polymorphisms in Pain Sensibility of Brazilian Fibromialgia Patients.” Rheumatology International, vol. 32, no. 2, Feb. 2012, pp. 427–30. PubMed, https://doi.org/10.1007/s00296-010-1659-z.Baumbauer, Kyle M., et al. “Contribution of COMT and BDNF Genotype and Expression to the Risk of Transition From Acute to Chronic Low Back Pain.” The Clinical Journal of Pain, vol. 36, no. 6, June 2020, pp. 430–39. PubMed Central, https://doi.org/10.1097/AJP.0000000000000819.Blancas-Flores, Gerardo, et al. “Glycine Suppresses TNF-α-Induced Activation of NF-κB in Differentiated 3T3-L1 Adipocytes.” European Journal of Pharmacology, vol. 689, nos. 1–3, Aug. 2012, pp. 270–77. PubMed, https://doi.org/10.1016/j.ejphar.2012.06.025.Checking Your Browser – reCAPTCHA. https://pmc.ncbi.nlm.nih.gov/articles/PMC9602431/. Accessed 2 July 2026.Chen, Jingshan, et al. “Functional Analysis of Genetic Variation in Catechol-O-Methyltransferase (COMT): Effects on mRNA, Protein, and Enzyme Activity in Postmortem Human Brain.” American Journal of Human Genetics, vol. 75, no. 5, Nov. 2004, pp. 807–21. PubMed, https://doi.org/10.1086/425589.Csiszar, Anna, Kira Smith, et al. “Resveratrol Attenuates TNF-Alpha-Induced Activation of Coronary Arterial Endothelial Cells: Role of NF-kappaB Inhibition.” American Journal of Physiology. Heart and Circulatory Physiology, vol. 291, no. 4, Oct. 2006, pp. H1694-1699. PubMed, https://doi.org/10.1152/ajpheart.00340.2006.Csiszar, Anna, Nazar Labinskyy, et al. “Vasoprotective Effects of Resveratrol and SIRT1: Attenuation of Cigarette Smoke-Induced Oxidative Stress and Proinflammatory Phenotypic Alterations.” American Journal of Physiology. Heart and Circulatory Physiology, vol. 294, no. 6, June 2008, pp. H2721–35. PubMed Central, https://doi.org/10.1152/ajpheart.00235.2008.Diatchenko, Luda, et al. “Genetic Basis for Individual Variations in Pain Perception and the Development of a Chronic Pain Condition.” Human Molecular Genetics, vol. 14, no. 1, Jan. 2005, pp. 135–43. PubMed, https://doi.org/10.1093/hmg/ddi013.Finan, Patrick H., et al. “COMT Moderates the Relation of Daily Maladaptive Coping and Pain in Fibromyalgia.” Pain, vol. 152, no. 2, Feb. 2011, pp. 300–07. PubMed, https://doi.org/10.1016/j.pain.2010.10.024.Firfirey, Firzana, et al. “Polymorphisms in COMT and OPRM1 Collectively Contribute to Chronic Shoulder Pain and Disability in South African Breast Cancer Survivors’.” Genes, vol. 14, no. 1, Dec. 2022, p. 9. PubMed Central, https://doi.org/10.3390/genes14010009.Hartung, Jane E., et al. “Β2- and Β3-Adrenergic Receptors Drive COMT-Dependent Pain by Increasing Production of Nitric Oxide and Cytokines.” Pain, vol. 155, no. 7, July 2014, pp. 1346–55. PubMed, https://doi.org/10.1016/j.pain.2014.04.011.Hussain, Saad Abdul-Rehman, et al. “Adjuvant Use of Melatonin for Treatment of Fibromyalgia.” Journal of Pineal Research, vol. 50, no. 3, Apr. 2011, pp. 267–71. PubMed, https://doi.org/10.1111/j.1600-079X.2010.00836.x.Jacobsen, L. M., et al. “The COMT Rs4680 Met Allele Contributes to Long-Lasting Low Back Pain, Sciatica and Disability after Lumbar Disc Herniation.” European Journal of Pain (London, England), vol. 16, no. 7, Aug. 2012, pp. 1064–69. PubMed, https://doi.org/10.1002/j.1532-2149.2011.00102.x.Jensen, Karin B., et al. “Increased Sensitivity to Thermal Pain Following a Single Opiate Dose Is Influenced by the COMT Val158met Polymorphism.” PLOS ONE, vol. 4, no. 6, June 2009, p. e6016. PLoS Journals, https://doi.org/10.1371/journal.pone.0006016.Jensen, Maureen C., et al. “Magnetic Resonance Imaging of the Lumbar Spine in People without Back Pain.” New England Journal of Medicine, vol. 331, no. 2, July 1994, pp. 69–73. DOI.org (Crossref), https://doi.org/10.1056/NEJM199407143310201.Lama, Adriano, et al. “Palmitoylethanolamide Dampens Neuroinflammation and Anxiety-like Behavior in Obese Mice.” Brain, Behavior, and Immunity, vol. 102, May 2022, pp. 110–23. PubMed, https://doi.org/10.1016/j.bbi.2022.02.008.Li, Wanjun, et al. “Pain in Parkinson’s Disease Associated with COMT Gene Polymorphisms.” Behavioural Neurology, vol. 2014, 2014, p. 304203. PubMed, https://doi.org/10.1155/2014/304203.Marini, Ida, et al. “Palmitoylethanolamide versus a Nonsteroidal Anti-Inflammatory Drug in the Treatment of Temporomandibular Joint Inflammatory Pain.” Journal of Orofacial Pain, vol. 26, no. 2, 2012, pp. 99–104.Martínez-Jauand, M., et al. “Pain Sensitivity in Fibromyalgia Is Associated with Catechol-O-Methyltransferase (COMT) Gene.” European Journal of Pain (London, England), vol. 17, no. 1, Jan. 2013, pp. 16–27. PubMed, https://doi.org/10.1002/j.1532-2149.2012.00153.x.Nackley, Andrea G., et al. “Low Enzymatic Activity Haplotypes of the Human Catechol-O-Methyltransferase Gene: Enrichment for Marker SNPs.” PLoS ONE, vol. 4, no. 4, Apr. 2009, p. e5237. PubMed Central, https://doi.org/10.1371/journal.pone.0005237.Nackley-Neely, Andrea Gail, et al. “Catechol-O-Methyltransferase Inhibition Increases Pain Sensitivity through Activation of Both Β2 and Β3 Adrenergic Receptors.” Pain, vol. 128, no. 3, Apr. 2007, pp. 199–208. PubMed Central, https://doi.org/10.1016/j.pain.2006.09.022.Nicholl, Barbara I., et al. “No Evidence for a Role of the Catechol-O-Methyltransferase Pain Sensitivity Haplotypes in Chronic Widespread Pain.” Annals of the Rheumatic Diseases, vol. 69, no. 11, Nov. 2010, pp. 2009–12. PubMed, https://doi.org/10.1136/ard.2009.126086.Schmahl, Christian, et al. “COMT Val158met Polymorphism and Neural Pain Processing.” PLOS ONE, vol. 7, no. 1, Jan. 2012, p. e23658. PLoS Journals, https://doi.org/10.1371/journal.pone.0023658.Schweiger, Vittorio, et al. “Ultramicronized Palmitoylethanolamide (Um-PEA) as Add-on Treatment in Fibromyalgia Syndrome (FMS): Retrospective Observational Study on 407 Patients.” CNS & Neurological Disorders Drug Targets, vol. 18, no. 4, 2019, pp. 326–33. PubMed, https://doi.org/10.2174/1871527318666190227205359.Segall, S. K., et al. “Janus Molecule I: Dichotomous Effects of COMT in Neuropathic vs Nociceptive Pain Modalities.” CNS & Neurological Disorders Drug Targets, vol. 11, no. 3, May 2012, pp. 222–35. PubMed Central, https://doi.org/10.2174/187152712800672490.Slade, G. D., A. E. Sanders, et al. “COMT Diplotype Amplifies Effect of Stress on Risk of Temporomandibular Pain.” Journal of Dental Research, vol. 94, no. 9, Sept. 2015, pp. 1187–95. PubMed Central, https://doi.org/10.1177/0022034515595043.Slade, G. D., R. B. Fillingim, et al. “COMT Genotype and Efficacy of Propranolol for TMD Pain: A Randomized Trial.” Journal of Dental Research, vol. 100, no. 2, Feb. 2021, pp. 163–70. PubMed Central, https://doi.org/10.1177/0022034520962733.Smith, Shad B., et al. “Epistasis Between Polymorphisms in COMT, ESR1, and GCH1 Influences COMT Enzyme Activity and Pain.” Pain, vol. 155, no. 11, Nov. 2014, pp. 2390–99. PubMed Central, https://doi.org/10.1016/j.pain.2014.09.009.Soultati, Ioanna, et al. “Effect of Common OPRM1, COMT, SLC6A4, ABCB1, and CYP2B6 Polymorphisms on Perioperative Analgesic and Propofol Demands on Patients Subjected to Thyroidectomy Surgery.” Pharmacological Reports, vol. 75, no. 2, 2023, pp. 386–96. PubMed Central, https://doi.org/10.1007/s43440-023-00455-7.Tchivileva, Inna E., et al. “Effect of Catechol-O-Methyltransferase Polymorphism on Response to Propranolol Therapy in Chronic Musculoskeletal Pain: A Randomized, Double–Blind, Placebo-Controlled, Crossover Pilot Study.” Pharmacogenetics and Genomics, vol. 20, no. 4, Apr. 2010, pp. 239–48. PubMed Central, https://doi.org/10.1097/FPC.0b013e328337f9ab.Wang, Liang-Jen, et al. “A Potential Interaction between COMT and MTHFR Genetic Variants in Han Chinese Patients with Bipolar II Disorder.” Scientific Reports, vol. 5, Mar. 2015, p. 8813. PubMed Central, https://doi.org/10.1038/srep08813.Xu, Ting, et al. “Oral Application of Magnesium-L-Threonate Attenuates Vincristine-Induced Allodynia and Hyperalgesia by Normalization of Tumor Necrosis Factor-α/Nuclear Factor-κB Signaling.” Anesthesiology, vol. 126, no. 6, June 2017, pp. 1151–68. PubMed, https://doi.org/10.1097/ALN.0000000000001601.Yalcin, Ipek, et al. “Chronic Treatment with Agonists of Beta(2)-Adrenergic Receptors in Neuropathic Pain.” Experimental Neurology, vol. 221, no. 1, Jan. 2010, pp. 115–21. PubMed, https://doi.org/10.1016/j.expneurol.2009.10.008.Yari, Zahra, et al. “The Effect of Hesperidin Supplementation on Metabolic Profiles in Patients with Metabolic Syndrome: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial.” European Journal of Nutrition, vol. 59, no. 6, Sept. 2020, pp. 2569–77. PubMed, https://doi.org/10.1007/s00394-019-02105-2.Zhang, Xin, et al. “Sustained Stimulation of Β2- and Β3-Adrenergic Receptors Leads to Persistent Functional Pain and Neuroinflammation.” Brain, Behavior, and Immunity, vol. 73, Oct. 2018, pp. 520–32. PubMed Central, https://doi.org/10.1016/j.bbi.2018.06.017.Zubieta, Jon-Kar, et al. “COMT Val158met Genotype Affects Mu-Opioid Neurotransmitter Responses to a Pain Stressor.” Science (New York, N.Y.), vol. 299, no. 5610, Feb. 2003, pp. 1240–43. PubMed, https://doi.org/10.1126/science.1078546.