Key takeaways:
- Choline is an essential nutrient that you get from your diet and also synthesize in your liver, which your body uses in several important ways.
- Choline is needed for brain function and cellular health. It can also be utilized in the methylation cycle as a methyl donor.
- Genetic variants can impact how well you create choline or how you convert between types of choline.
- Studies show that genetic variants significantly impact how much choline you need from your diet in order to maintain adequate supplies.
- Personalize your choline based on your genetic variants: PEMT T/T carriers benefit most from supplementation, while BHMT A carriers may prefer choline over betaine. Slow COMT may also interact with betaine supplements.
Choline: From brain health to gut health
The best type of choline for you depends on your genetic variants in PEMT, MTHFD1, and CHKA genes, plus your TMAO concerns. Optimizing your choline intake can help your brain function, heart health, mood, and more.
Let’s dive into the science on choline – what it is, how it is synthesized, and how it is used.
What is choline?
Choline is a vitamin-like nutrient used in every cell of your body. As with most truly essential biological processes, we have redundant pathways to ensure choline availability. While some choline can be synthesized in cells, without the additional choline you get from your diet, these synthesis pathways can’t keep up.
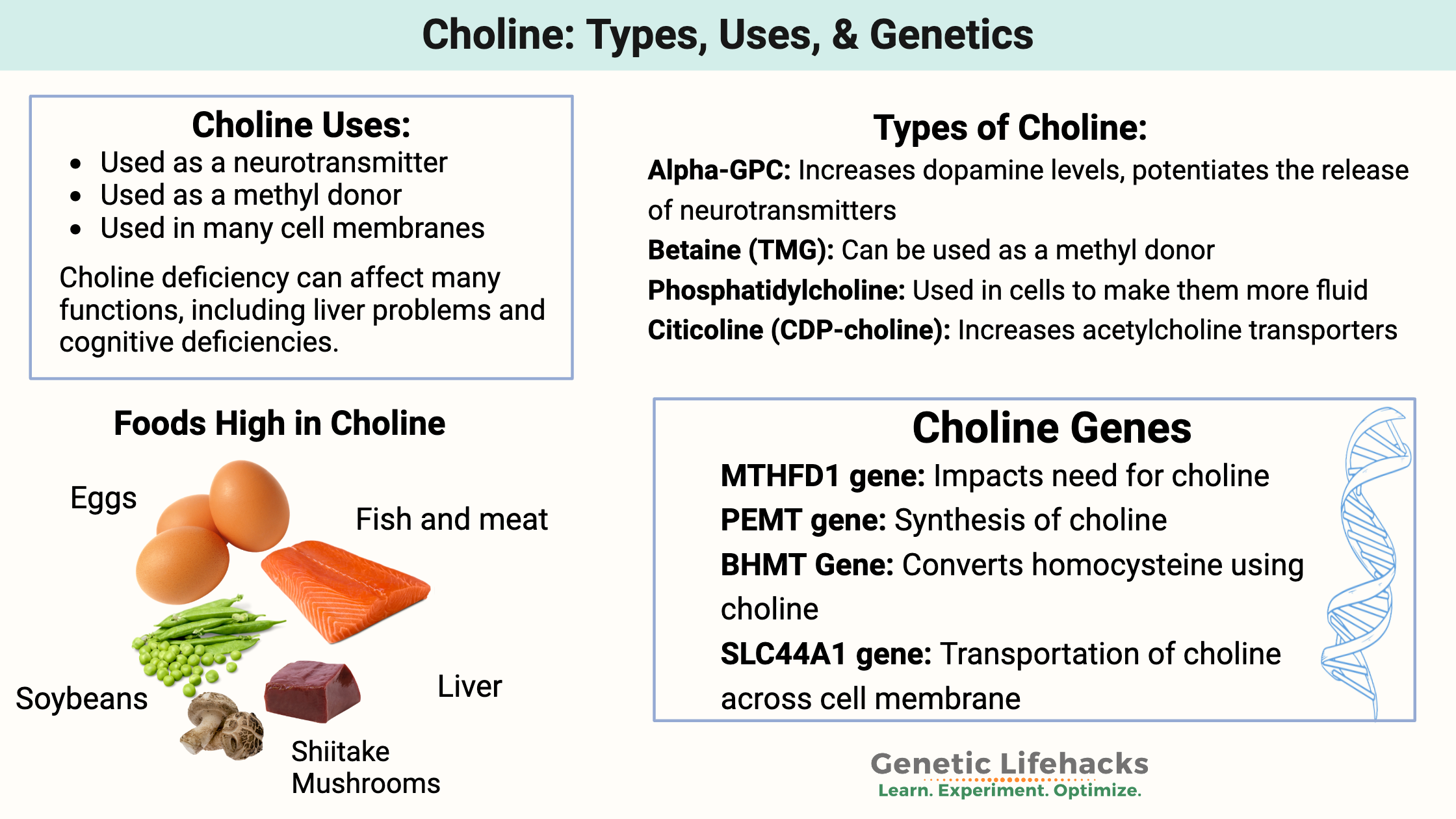
Choline is the precursor used for phosphatidyl choline, which is part of every cell membrane, acetylcholine (neurotransmitter), and betaine (methyl donor). So choline touches every cell in the body and is foundational for cholinergic neurotransmission.
What happens without enough choline?
Choline deficiency can cause symptoms ranging from cognitive problems to muscle weakness to mood changes to fatty liver disease. Choline deficiency also affects cholesterol secretion from the liver, which can limit the amount of circulating cholesterol (used for vitamin D and hormones). In pregnancy, choline deficiency increases the risk of neural tube defects and affects brain development in the baby.[ref]
What do the different types of choline do in the body?
Choline converts into three main forms: betaine (a methyl donor), acetylcholine (a neurotransmitter for memory and learning), and phosphatidylcholine (for cell membrane health).[ref]
- Betaine (TMG): Oxidized form of choline that can be used as a methyl donor.
- Acetylcholine: An acetylated form of choline used extensively as a neurotransmitter in the brain and peripheral neurons. It is essential for learning, attention, and memory.
- Phosphatidylcholine: Incorporated into all of your cell membranes to make them more fluid and function properly.
Tradeoffs to consider as we dig into the research:
Choline is necessary in the right amount. Not enough choline impacts cognitive function, reproduction, and liver function. On the other hand, too much choline may interact with the gut microbiome to produce a choline-derived metabolite (TMAO), which is linked to an increased risk of heart disease. (More on this in a minute)[ref]
How Your Body Makes Choline
Your body makes choline, but not at sufficient levels to meet all of your needs. This is why choline is considered an essential nutrient — we need to get at least part of our daily requirements from food.
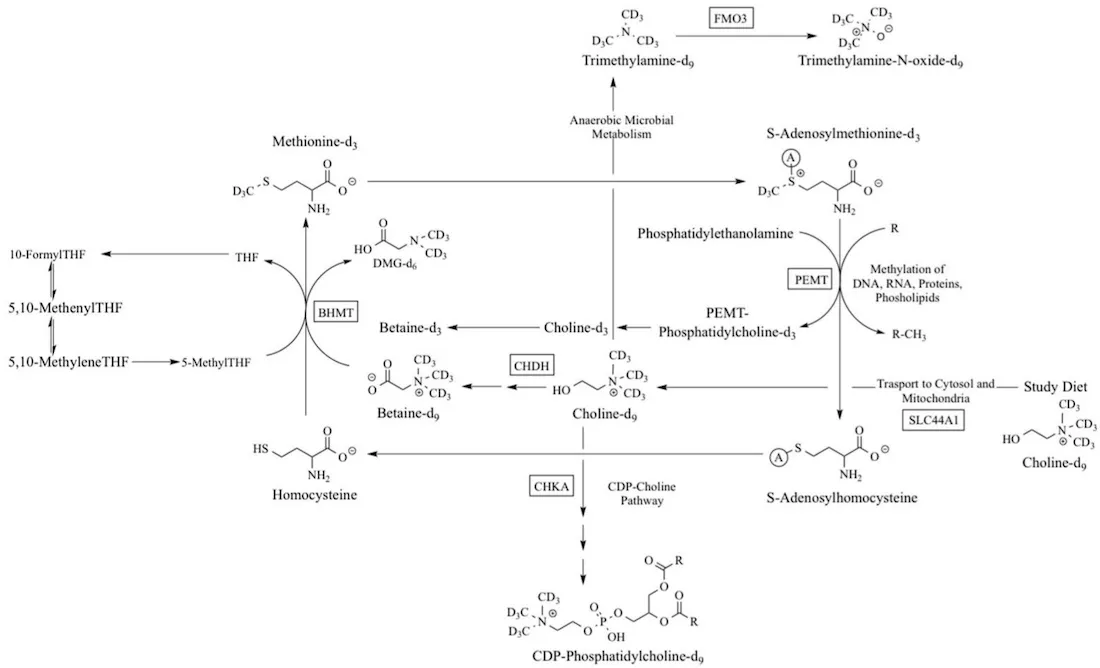
In the liver, the PEMT enzyme converts phosphatidylethanolamine into phosphatidylcholine (PC) with the addition of a methyl group. Choline synthesis in the body depends both on having enough of the PEMT enzyme (genetics) as well as sufficient methyl groups (diet, genetics) — along with methionine (amino acid, abundant in high protein foods).
Related articles: MTHFR variants | Methylation cycle genes
Here’s an overview of the biochemical pathways for choline synthesis. The genes involved are in rectangular boxes.
Choline recommendations:
The daily recommended adequate intake (AI) of choline is 550 mg for men and 425mg for women.
The AI for choline may not be enough for everyone, though. In one study, some men developed signs of liver damage when restricted to only 550 mg/day of choline.[ref] Other studies point to genetic variants and ancestry as impacting the dietary requirement for choline.[ref]
The Choline Information Council states that 90% of people in the US are choline deficient.
Can you take too much choline?
The upper limit recommendation is 3500 mg/day. Taking too much choline can lead to choline toxicity and a fishy body odor.
How quickly can you run out of choline?
A research study in the early 90s had healthy male volunteers eat a diet containing no choline for three weeks, along with adequate, but not excess, methionine. The liver can make some choline with methionine. The results showed “plasma choline and phosphatidylcholine concentrations decreased an average of 30% during the 3-week period when a choline-deficient diet was ingested”. Liver enzyme tests showed that there were signs of liver dysfunction beginning.[ref]
A follow-up study was done with both men and women on a low-choline (50 mg/day) diet. The study lasted either 42 days or until signs of organ failure(!), whichever came first. The results showed that men and postmenopausal women were more likely to have organ damage faster than premenopausal women, indicating that estrogen may play a role in how the body prioritizes choline creation.[ref]
Indeed, later research shows that an estrogen response element directly affects PEMT expression.[ref] Thus, women who are premenopausal induce PEMT and create choline at higher levels. This is likely due to choline being essential in reproduction. It protects the fetus if the mother’s diet lacks choline, which was a situation often faced by our ancestors with seasonal deficiencies.
Choline for the brain:
When you look at supplemental choline products, such as citicoline or Alpha-GPC, you’ll find that some are marketed as nootropics that supposedly increase focus and memory. Sounds great, but how does this work?
Let’s dig into what choline is doing in the brain and elsewhere…
Memory, attention, motivation:
Acetylcholine is chemically defined as an ester of acetic acid and choline. Acetylcholine acts as a neurotransmitter in the brain, signaling from one neuron to another. Acetylcholine-activated brain regions are important in attention, memory, arousal, and motivation.[ref]
Rest and digest (parasympathetic):
The parasympathetic nervous system uses acetylcholine almost exclusively as the neurotransmitter. The parasympathetic nervous system is responsible for the autonomic actions that you don’t have to think about – digestion, salivation, urination, tears, eye movement, and heart rhythm (at rest). Motor neurons also use acetylcholine to activate muscles. Thus, acetylcholine touches on a lot of different systems in the body.
Menopausal brain changes:
A 2026 study in the journal Nutrients looked at the effects of supplemental choline on the cognitive problems often experienced in menopause. The expression of PEMT is influenced by estrogen levels, so the changes in estrogen at menopause can decrease the amount of choline available to the brain. MRI scans and functional connectivity tests showed that choline likely influences working memory in menopause.[ref] A prior study showed that higher dietary choline and betaine intake was associated with slower cognitive decline in women as they age.[ref] Thus, for women experiencing brain fog in menopause, increasing dietary choline or supplementing with choline may be beneficial.
When looking at changes in the brain from choline, researchers use animal models to trace what is happening.
- Animal studies show that choline, specifically Alpha-GPC, potentiates the release of neurotransmitters in the hippocampus. Alpha-GPC also increased striatal dopamine levels, likely by increasing acetylcholine availability.[ref][ref]
- Both CDP-choline (citicoline) and Alpha-GPC increase acetylcholine transporters and acetylcholine synthesis in the brain.[ref]
Should You Worry About TMAO from Choline?
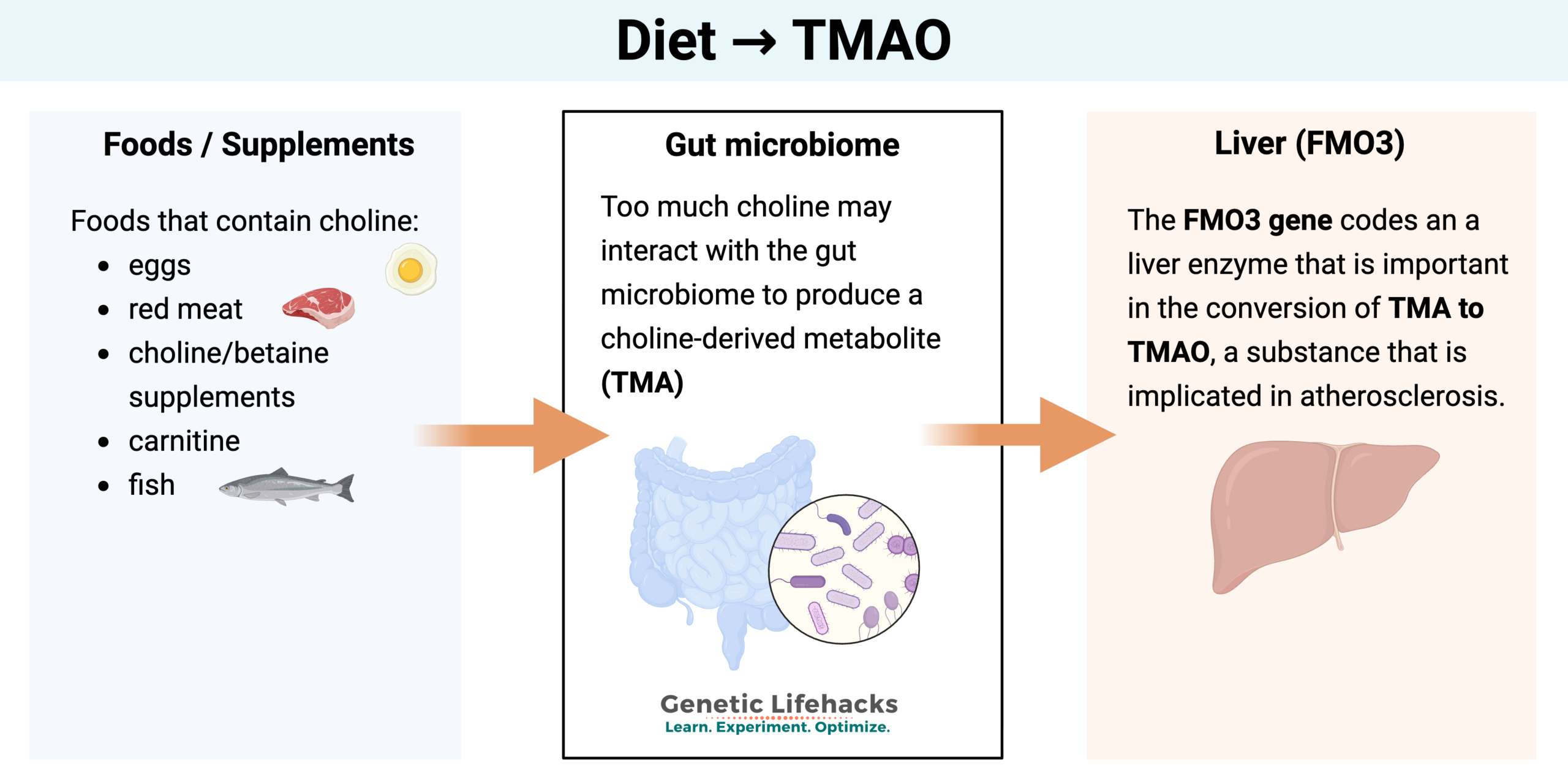
I mentioned above that the drawback to higher choline intake is the creation of TMAO. Trimethylamine N-oxide (TMAO) is a molecule generated by gut bacteria from choline, betaine, and carnitine. Recently, studies have correlated high TMAO levels with heart disease and possibly neurological disorders.
Let’s look at how TMAO is made:
In the gut, bacteria can turn choline, betaine, L-carnitine, ergothioneine (from mushrooms), and other choline-containing compounds into trimethylamine N-oxide (TMA). Additionally, TMA and TMAO can be found in fish.
TMA from food and gut bacteria is rapidly absorbed in the intestines and travels to the liver. The FMO3 enzyme converts TMA to TMAO.
Related article: FMO3 genetic variants
Factors influencing TMAO formation include older age, high-fat Western diet, diabetes, and the gut microbiome. Diet alters FMO3 activity, with Brassica vegetables, such as cabbage or broccoli, decreasing FMO3 and thus lowering TMAO. In addition, the gut microbiome affects TMA production, and the amount of fiber in the diet can alter the gut microbiome.[ref]
In general, older people and people who eat a typical, high-fat Western diet have higher levels of TMAO — and are more likely to have atherosclerosis and heart disease. The question of whether high TMAO causes heart disease is still being studied. While there is an association, it is harder to prove that TMAO causes heart attacks due to comorbidities and confounders. For example, TMAO levels are higher in people with diabetes, metabolic syndrome, or kidney problems. All of these are also risk factors for heart disease.[ref] Genetic studies also show that diabetes and kidney disease-related genetic variants may be causing the increase in TMAO, further confounding the correlation between TMAO and cardiovascular disease.[ref]
A 2026 study involving healthy adult males showed an interesting dietary connection. The 6-week trial involved half (n=51) of the men eating red meat, which contains choline. The other half of the participants swapped in beans for their protein source. After six weeks, the bean group had lower plasma choline levels, but they had no change in TMAO levels or inflammatory markers.[ref]
On the other hand, animal studies show a link between TMAO levels and heart dysfunction. Moreover, blocking the formation of TMAO while keeping the same diet prevented cardiac dysfunction.[ref] Cell studies show that TMAO increases vascular cell adhesion molecule-1, which is implicated in atherosclerosis.[ref]
While there is still a lot of research needed here, to err on the side of caution, you likely want to avoid TMAO being high.
Let’s switch gears and look at your genes and then the specifics of how your genes influence which type of choline may work best.
Choline Genotype Report
Access this content:
An active subscription is required to access this content.
Lifehacks:
All of this information about how the body uses choline is great, but I bet you are now wondering, “How do I use it?”.
Choline-rich foods vs. supplements:
The AI (adequate intake) of choline is set at 550 mg/day for men and 425-450/day for women (higher for pregnancy). The upper limit recommendation is 3500 mg/day. About 90% of people in the US don’t meet even the AI through their normal diet.[ref]
First, figure out how much choline you consume on average. Cronometer.com is a free web app for tracking micro and macronutrients. Choline isn’t included in the standard view, but you can go into the settings and include it. Track your food for a few days and see what you consume. For example, if you’re eating liver regularly, you are likely getting enough choline, but for liver-haters, it can be tough.
Foods high in choline include:
- liver
- egg yolks
- bacon
- beef
- pork
- soybeans
- wheat germ
Related article: Choline-rich foods and recipes
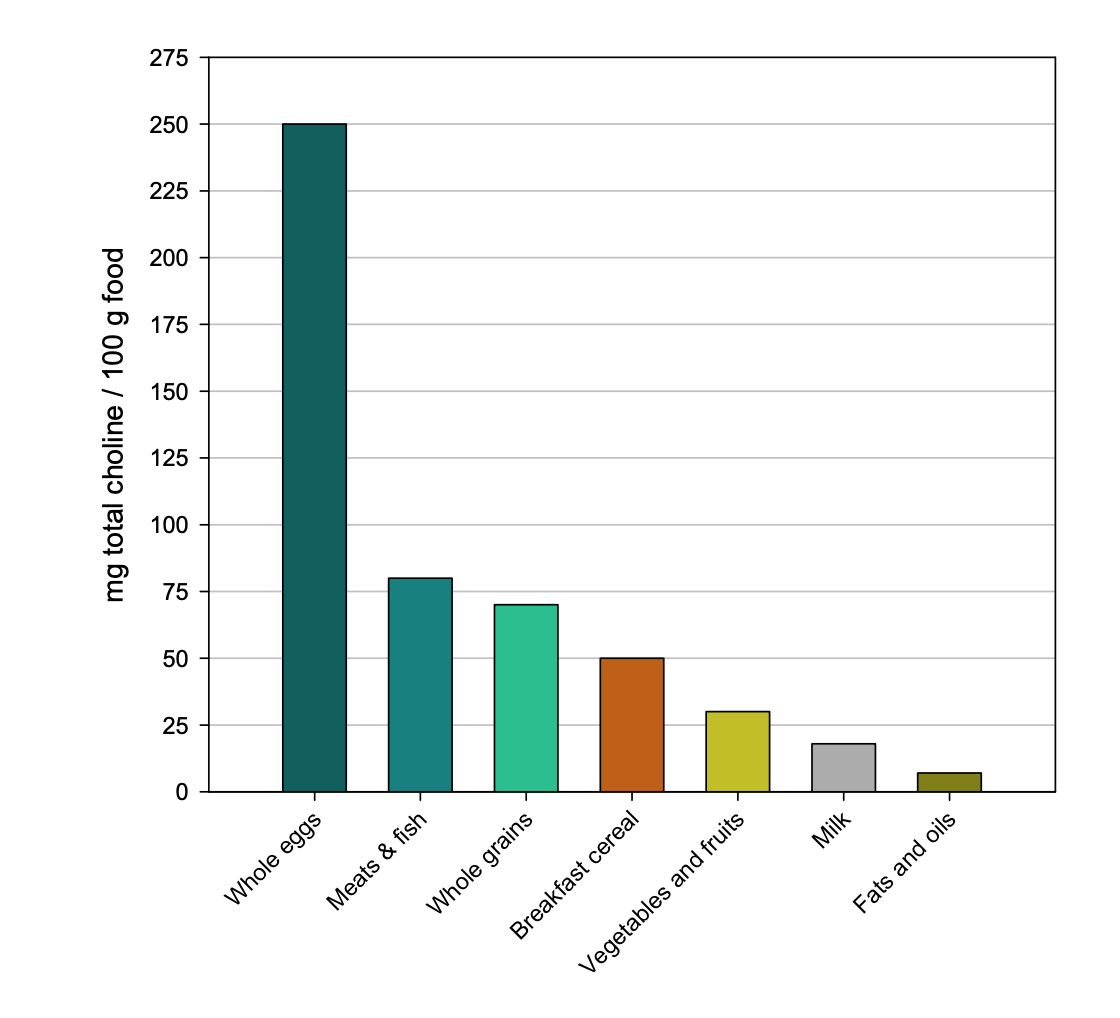
For most populations, eggs are the primary dietary source of choline. High-fiber bread (wheat germ) is the main dietary source of betaine.[ref]
Eggs are better:
A research study looked at choline uptake from foods vs. supplemental choline bitartrate. The plasma choline response was four times higher after consuming egg yolks with 3g of choline compared with a choline bitartrate supplement with 3g of choline.[ref]
Another study looked at betaine supplementation vs. betaine and/or choline from foods. All increased choline levels and decreased homocysteine.[ref]
TMAO considerations:
Testing: If you have concerns about heart disease and are worried that choline will make it worse, a TMAO test can help determine your current levels. A cardiologist may order the test for you, or you can order it yourself in the US for around $100.
Related article: Ordering your own labs and blood tests
Resveratrol: A clinical trial shows that a polyphenol formula with resveratrol decreased TMAO levels by 62% in 4 weeks.[ref]
Related article: Resveratrol: Genetic Interactions and Bioavailability
Phosphatidylcholine: One study showed that choline bitartrate increased TMAO levels quite a bit, however, phosphatidylcholine supplementation did not increase TMAO compared to baseline.[ref] Thus, if you are concerned about TMAO, phosphatidylcholine supplements or phosphatidylcholine in foods is likely a safer option for you.
Safety of supplemental choline:
The tolerable recommended upper intake level for choline is set at 3,500 mg/day for adults. Studies show that at doses of 10,000 – 16,000 mg/day, some people will have an odd, fishy odor due to the excretion of trimethylamine. Another study showed that at 7,500 mg/day, there is a slight blood pressure-lowering effect.[ref]
A 2021 study on adults prescribed to take choline (alpha-GPC) found a correlation between increased stroke risk and taking alpha-GPC. However, the confounding bias here is that the reason for prescribing alpha-GPC was to prevent or slow down cognitive decline or dementia.[ref] However, the possible increase in relative stroke risk is something to take into consideration with higher levels of alpha-GPC supplements in older adults.
What is the best type of choline for MTHFR mutations?
This is a question that comes up a lot. Supplementing with betaine directly increases the availability of methyl groups, but it doesn’t necessarily give you the wider benefits seen with increasing choline. A clinical trial involving equivalent doses in the form of choline chloride, choline bitartrate, α-GPC choline, and egg phosphatidylcholine looked at the plasma choline and betaine levels. All forms raised both plasma choline and betaine levels equally, and TMAO increased with all forms except for egg phosphatidylcholine.[ref] Thus, all types of choline are helpful for people with MTHFR variants.
Related article: MTHFR genetic variants
Different Types of Supplemental Choline:
Types of choline supplements include:
- CDP-choline (Citicoline)
- Alpha-GPC choline
- phosphatidylcholine
- betaine (TMG, trimethylglycine)
- choline bitartrate
Things to consider when choosing supplemental choline include the conversion to TMAO, the absorption and utilization, and the source. Many phosphatidylcholine supplements are made from soy, which some people want to avoid.
| Choline Type | Bioavailability | TMAO Risk | Best For | Genetic Considerations |
|---|---|---|---|---|
| Citicoline | High | Low | Memory, focus, stroke recovery | Works well for PCYT1A variants |
| Alpha-GPC | Very High | Moderate-High | Athletic performance, dementia | Avoid at higher levels if concerned about stroke risk |
| Phosphatidylcholine | Moderate | Low | Liver health, cell membranes | Good for all genotypes |
| Betaine (TMG) | High | N/A | Methylation support | Avoid high doses with slow COMT (A/A) |
| Choline Bitartrate | Moderate | High | Budget option | Increases TMAO significantly |
Let’s look at each type of choline and the genetic connections:
Citicoline
Access this content:
An active subscription is required to access this content.
Related B Vitamins and Methylation
Related Articles and Topics:
Specialized Pro-resolving Mediators (SPMs): The Resolution of Inflammation
References:
Bale, Govardhan, et al. “Whole-Exome Sequencing Identifies a Variant in Phosphatidylethanolamine N-Methyltransferase Gene to Be Associated with Lean-Nonalcoholic Fatty Liver Disease.” Journal of Clinical and Experimental Hepatology, vol. 9, no. 5, Oct. 2019, pp. 561–68. https://doi.org/10.1016/j.jceh.2019.02.001.
Böckmann, Katrin A., et al. “Differential Metabolism of Choline Supplements in Adult Volunteers.” European Journal of Nutrition, vol. 61, no. 1, Feb. 2022, pp. 219–30. https://doi.org/10.1007/s00394-021-02637-6.
Chen, Kui, et al. “Gut Microbiota-Dependent Metabolite Trimethylamine N-Oxide Contributes to Cardiac Dysfunction in Western Diet-Induced Obese Mice.” Frontiers in Physiology, vol. 8, 2017. https://doi.org/10.3389/fphys.2017.00139.
Chmurzynska, Agata, et al. “PEMT Rs12325817 and PCYT1A Rs7639752 Polymorphisms Are Associated with Betaine but Not Choline Concentrations in Pregnant Women.” Nutrition Research, vol. 56, Aug. 2018, pp. 61–70. https://doi.org/10.1016/j.nutres.2018.04.018.
Christensen, Karen E., et al. “The MTHFD1 p.Arg653Gln Variant Alters Enzyme Function and Increases Risk for Congenital Heart Defects.” Human Mutation, vol. 30, no. 2, Feb. 2009, pp. 212–20. https://doi.org/10.1002/humu.20830.
da Costa, Kerry-Ann, Olga G. Kozyreva, et al. “Common Genetic Polymorphisms Affect the Human Requirement for the Nutrient Choline.” The FASEB Journal, vol. 20, no. 9, July 2006, pp. 1336–44. https://doi.org/10.1096/fj.06-5734com.
da Costa, Kerry-Ann, Karen D. Corbin, et al. “Identification of New Genetic Polymorphisms That Alter the Dietary Requirement for Choline and Vary in Their Distribution across Ethnic and Racial Groups.” The FASEB Journal, vol. 28, no. 7, July 2014, pp. 2970–78. https://doi.org/10.1096/fj.14-249557.
Dumas, Julie A., et al. “Oral Choline Reduced Working Memory-Related Brain Activation in Postmenopausal Women: A Pilot Study.” Nutrients, vol. 18, no. 3, Jan. 2026, p. 459. https://doi.org/10.3390/nu18030459.
Fischer, Leslie M., Kerry-Ann da Costa, et al. “Dietary Choline Requirements of Women: Effects of Estrogen and Genetic Variation.” The American Journal of Clinical Nutrition, vol. 92, no. 5, Nov. 2010, p. 1113. https://doi.org/10.3945/ajcn.2010.30064.
Fischer, Leslie M., Kerry Ann daCosta, et al. “Sex and Menopausal Status Influence Human Dietary Requirements for the Nutrient Choline.” The American Journal of Clinical Nutrition, vol. 85, no. 5, May 2007, pp. 1275–85. https://doi.org/10.1093/ajcn/85.5.1275.
Ganz, Ariel B., Kevin C. Klatt, et al. “Common Genetic Variants Alter Metabolism and Influence Dietary Choline Requirements.” Nutrients, vol. 9, no. 8, Aug. 2017, p. 837. https://doi.org/10.3390/nu9080837.
Ganz, Ariel B., Vanessa V. Cohen, et al. “Genetic Variation in Choline-Metabolizing Enzymes Alters Choline Metabolism in Young Women Consuming Choline Intakes Meeting Current Recommendations.” International Journal of Molecular Sciences, vol. 18, no. 2, Feb. 2017. https://doi.org/10.3390/ijms18020252.
Grieb, Pawel. “Neuroprotective Properties of Citicoline: Facts, Doubts and Unresolved Issues.” CNS Drugs, vol. 28, no. 3, 2014, p. 185. https://doi.org/10.1007/s40263-014-0144-8.
Janeiro, Manuel H., et al. “Implication of Trimethylamine N-Oxide (TMAO) in Disease: Potential Biomarker or New Therapeutic Target.” Nutrients, vol. 10, no. 10, Oct. 2018. https://doi.org/10.3390/nu10101398.
Jia, Jinzhu, et al. “Assessment of Causal Direction Between Gut Microbiota-Dependent Metabolites and Cardiometabolic Health: A Bidirectional Mendelian Randomization Analysis.” Diabetes, vol. 68, no. 9, Sept. 2019, pp. 1747–55. https://doi.org/10.2337/db19-0153.
Kapalka, George M. “Substances Involved in Neurotransmission.” Nutritional and Herbal Therapies for Children and Adolescents, edited by George M. Kapalka, Academic Press, 2010, pp. 71–99. https://doi.org/10.1016/B978-0-12-374927-7.00004-2.
Kohlmeier, Martin, et al. “Genetic Variation of Folate-Mediated One-Carbon Transfer Pathway Predicts Susceptibility to Choline Deficiency in Humans.” Proceedings of the National Academy of Sciences of the United States of America, vol. 102, no. 44, Nov. 2005, pp. 16025–30. https://doi.org/10.1073/pnas.0504285102.
Konstantinova, Svetlana V., et al. “Dietary Patterns, Food Groups, and Nutrients as Predictors of Plasma Choline and Betaine in Middle-Aged and Elderly Men and Women.” The American Journal of Clinical Nutrition, vol. 88, no. 6, Dec. 2008, pp. 1663–69. https://doi.org/10.3945/ajcn.2008.26531.
Ma, GuoHua, et al. “Trimethylamine N-Oxide in Atherogenesis: Impairing Endothelial Self-Repair Capacity and Enhancing Monocyte Adhesion.” Bioscience Reports, vol. 37, no. 2, Apr. 2017. https://doi.org/10.1042/BSR20160244.
Mueller, Daniel M., et al. “Plasma Levels of Trimethylamine-N-Oxide Are Confounded by Impaired Kidney Function and Poor Metabolic Control.” Atherosclerosis, vol. 243, no. 2, Dec. 2015, pp. 638–44. https://doi.org/10.1016/j.atherosclerosis.2015.10.091.
Ren, Bingnan, et al. “Association between the BHMT Gene Rs3733890 Polymorphism and the Efficacy of Oral Folate Therapy in Patients with Hyperhomocysteinemia.” Annals of Human Genetics, vol. 83, no. 6, Nov. 2019, pp. 434–44. https://doi.org/10.1111/ahg.12326.
Schettini, G., et al. “Molecular Mechanisms Mediating the Effects of L-Alpha-Glycerylphosphorylcholine, a New Cognition-Enhancing Drug, on Behavioral and Biochemical Parameters in Young and Aged Rats.” Pharmacology, Biochemistry, and Behavior, vol. 43, no. 1, Sept. 1992, pp. 139–51. https://doi.org/10.1016/0091-3057(92)90650-5.
Smallwood, Tangi, et al. “Choline Metabolites: Gene by Diet Interactions.” Current Opinion in Lipidology, vol. 27, no. 1, Feb. 2016, p. 33. https://doi.org/10.1097/MOL.0000000000000259.
Smolders, Lotte, et al. “Natural Choline from Egg Yolk Phospholipids Is More Efficiently Absorbed Compared with Choline Bitartrate; Outcomes of a Randomized Trial in Healthy Adults.” Nutrients, vol. 11, no. 11, Nov. 2019. https://doi.org/10.3390/nu11112758.
Synoradzki, Kamil, and Paweł Grieb. “Citicoline: A Superior Form of Choline?” Nutrients, vol. 11, no. 7, July 2019. https://doi.org/10.3390/nu11071569.
Tan, Hwa-Li, et al. “Phosphatidylethanolamine N-Methyltransferase Gene Rs7946 Polymorphism Plays a Role in Risk of Nonalcoholic Fatty Liver Disease: Evidence from Meta-Analysis.” Pharmacogenetics and Genomics, vol. 26, no. 2, Feb. 2016, pp. 88–95. https://doi.org/10.1097/FPC.0000000000000193.
Tayebati, Seyed Khosrow, et al. “Effect of Choline-Containing Phospholipids on Brain Cholinergic Transporters in the Rat.” Journal of the Neurological Sciences, vol. 302, no. 1–2, Mar. 2011, pp. 49–57. https://doi.org/10.1016/j.jns.2010.11.028.
Trabucchi, M., et al. “Changes in the Interaction between CNS Cholinergic and Dopaminergic Neurons Induced by L-Alpha-Glycerylphosphorylcholine, a Cholinomimetic Drug.” Il Farmaco; Edizione Scientifica, vol. 41, no. 4, Apr. 1986, pp. 325–34.
Zafonte, Ross D., et al. “Effect of Citicoline on Functional and Cognitive Status among Patients with Traumatic Brain Injury: Citicoline Brain Injury Treatment Trial (COBRIT).” JAMA, vol. 308, no. 19, Nov. 2012, pp. 1993–2000. https://doi.org/10.1001/jama.2012.13256.
Zeisel, Steven H., et al. “Choline, an Essential Nutrient for Humans.” The FASEB Journal, vol. 5, no. 7, Apr. 1991, pp. 2093–98. https://doi.org/10.1096/fasebj.5.7.2010061.