Key takeaways:
- Creatine acts as a backup energy source for muscles and the brain to use in times of stress.
- Genetic variants in the genes related to creatine synthesis, including GATM and CKM, can impact muscle pain, athletic performance, and cognitive ability.
- Creatine supplements are inexpensive and readily available. Studies show that creatine monohydrate supplementation effectively boosts muscle power and brain creatine levels under certain conditions.
What is creatine?
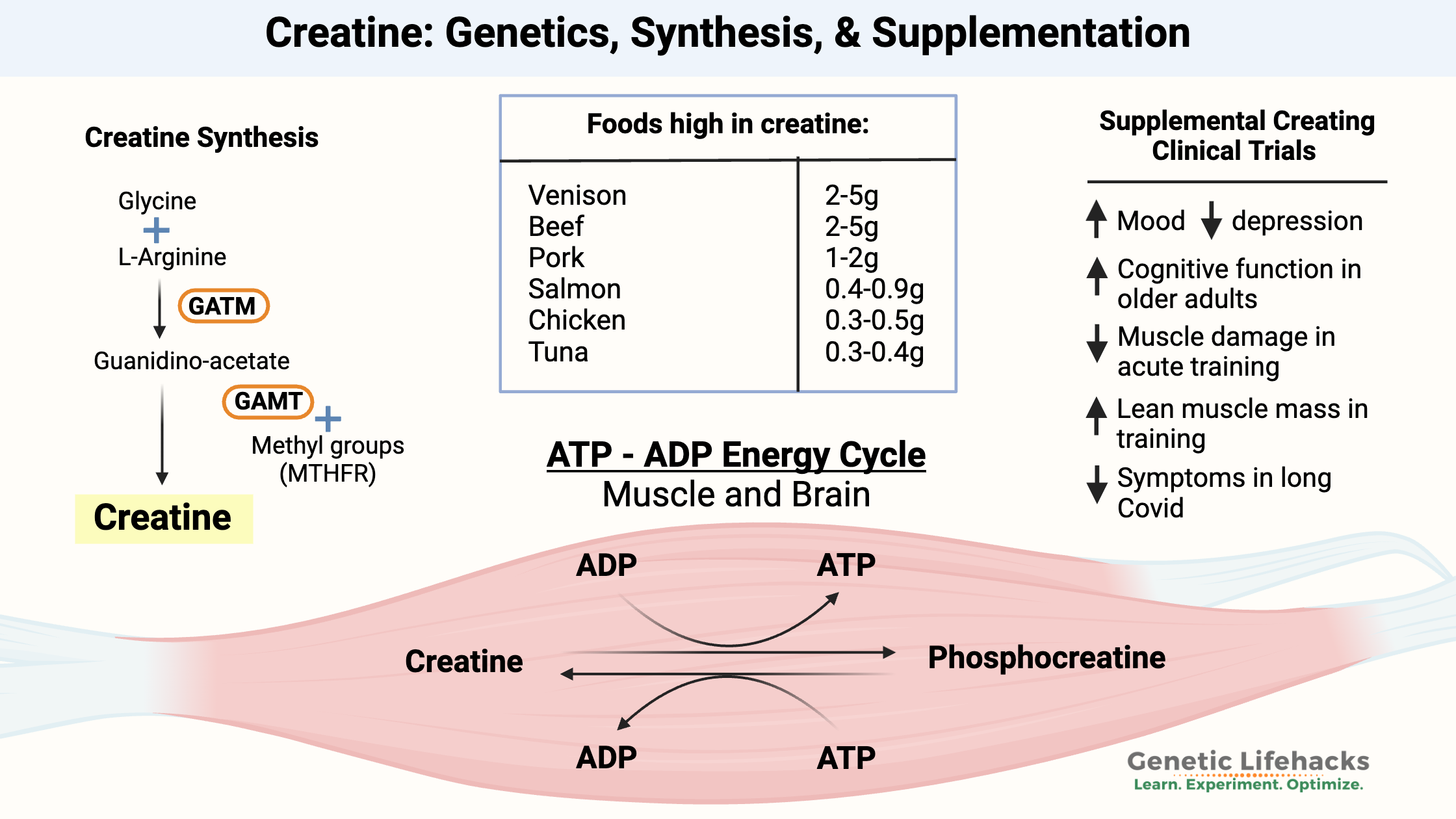
Creatine is a molecule synthesized from amino acids that plays an important role in energy production within both brain tissue and muscles. The body can synthesize creatine from other amino acids, and you can get it from your diet.
Let’s first take a look at how creatine is used in cellular energy:
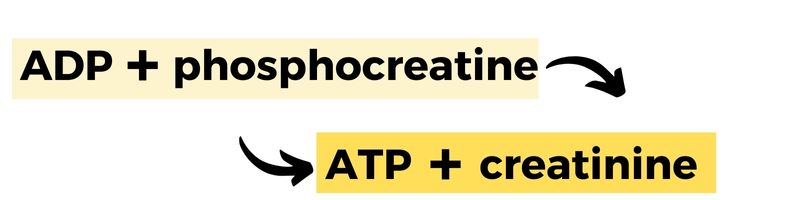
Adenosine triphosphate (ATP) is at the heart of cellular energy. ATP is primarily produced in mitochondria — you know, the powerhouse of the cell. ATP stores energy in the bonds between the phosphates, which store and then can release energy within the cell.
The ‘triphosphate’ part of ATP means it has three phosphates bound together. When ATP releases energy, it sheds one of its phosphates and becomes adenosine diphosphate (ADP) with only two phosphates remaining.
This is where creatine comes in. In specific cell types, creatine helps recycle ADP back into ATP by donating a phosphate group. Thus, creatine can help replenish cellular energy when it’s running low.
How does the body make creatine?
Creatine is synthesized from the amino acids glycine and arginine, along with a methyl group donated by SAMe.
The biosynthesis of creatine is a multi-step process.
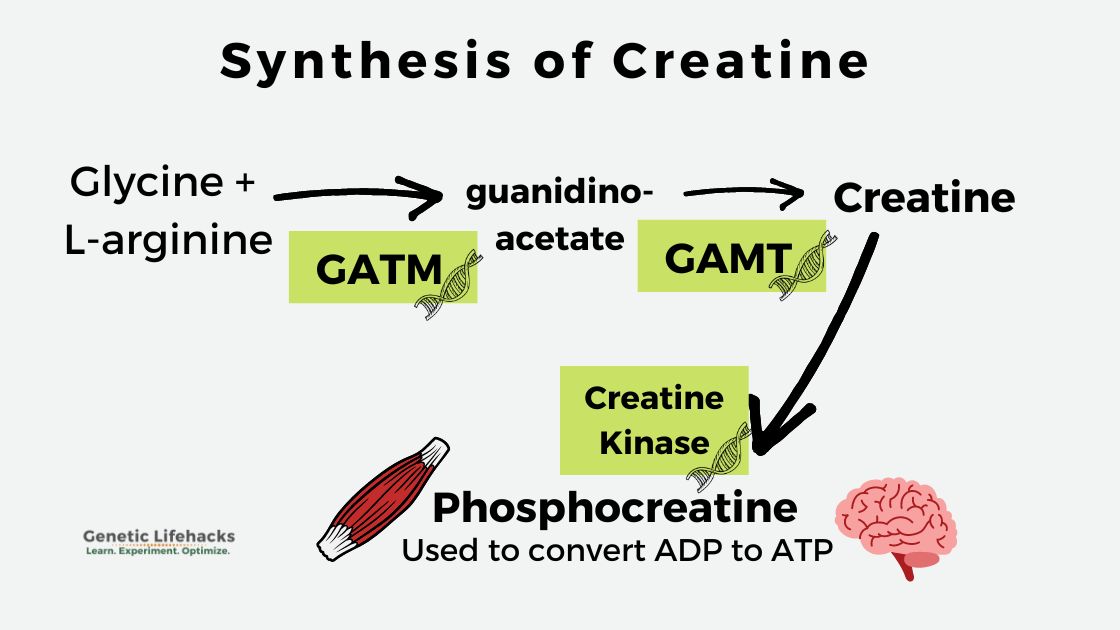
First, glycine and arginine, two common amino acids, combine to form guanidinoacetate. Then, creatine is formed from guanidinoacetate with the addition of a methyl group. This process occurs primarily in the liver and kidneys. Once synthesized, creatine then enters the bloodstream and can be used throughout the body.[ref]
Within cells, creatine can be further converted to phosphocreatine with the help of the enzyme creatine kinase (CK). Phosphocreatine, also known as creatine phosphate, stands ready, available for converting ADP to ATP when more energy is needed.
Muscle cells and the brain both need a lot of ATP for energy. When a lot of energy is required, such as lifting something heavy or sprinting, phosphocreatine rapidly replenishes ATP from ADP. In normal, lower-energy situations, ATP is produced directly from glucose or fatty acids.
In addition to being synthesized in the liver, creatine can be obtained from the diet as well as from supplements. Creatine is naturally found in animal protein-rich foods, such as muscle meats. Supplemental creatine, which bodybuilders commonly use, is also a source of creatine for creating the phosphocreatine used when repairing and building muscles.
Diving deeper into creatine kinase:
I mentioned above that creatine kinase is the enzyme used to convert creatine to phosphocreatine, which can then be used by cells for energy when needed.
There are two types of creatine kinase – mitochondrial and cytosolic – found in the muscle and brain. The phosphocreatine created in the reaction acts as an energy buffer, readily available when muscle cells are stressed and need a burst of ATP for energy.[ref]
In medical contexts, doctors often measure creatine kinase levels in the blood to assess tissue damage, especially in cases like cardiac muscle damage during a heart attack. When tissues are harmed, creatine kinase can leak into the bloodstream, serving as a valuable indicator.
Lab tests for creatine kinase:
Doctors often measure creatine kinase levels in the blood to assess tissue damage. For example, if cardiac muscle is damaged during a heart attack, creatine kinase levels will usually be elevated.[ref] CK levels increase in response to brain, heart, or muscle damage.[ref]
What else elevates creatine kinase (CK) levels on tests?
Aside from heart attacks, strenuous exercise can elevate CK levels up to 15 times the normal level. For instance, after running a marathon, CK levels peak after 24 hours and remain elevated for a week.[ref]
Additional causes of elevated CK levels:
- Statins can raise CK levels in people who have statin-induced muscle pain.[ref]
- Obesity or African ancestry is associated with higher CK levels.[ref]
How is creatine used in the body?
While creatine supplements are typically associated with bodybuilders, it is actually utilized throughout the body. I’m going to dive into the details on specific ways that creatine is used in different systems of the body, and then cover the clinical trials on supplemental creatine.
| Tissue/Organ | Role of Creatine | Special Notes |
|---|---|---|
| Muscle | Rapid ATP regeneration during high-intensity work | Major site of creatine storage |
| Brain | Energy buffer, supports cognitive function | May require higher intake for effect |
| Adipose (fat) | Supports thermogenesis, energy expenditure | Important in brown/beige fat, metabolic health |
| Heart | Energy supply, marker for tissue damage | CK levels used clinically |
Creatine and Brain Function:
The brain, despite its relatively small size, uses up a ton of energy (ATP) in comparison with the rest of the body.
In the brain, creatine serves as an energy buffer to provide energy in times of stress.[ref] Genetic mutations that cause creatine deficiency in the brain result in severe developmental disorders and seizures.
Creatine obtained from diet or supplements can cross the blood-brain barrier, but the amount that reaches the brain is generally less than what is absorbed by muscles. This implies that to positively impact brain function, a higher intake of creatine might be necessary. Alternatively, it could mean that creatine is prioritized by the muscles unless there is an urgent requirement for it to go to the brain.
As one research study puts it: “It could be that the brain relies primarily on endogenous creatine synthesis until there is some sort of challenge to brain creatine status. These challenges, which could cause a decrease in brain creatine, could be acute (e.g., sleep deprivation, intense exercise) or chronic (e.g., aging, traumatic brain injury, depression, Alzheimer’s disease, creatine synthesis enzyme deficiencies).”[ref]
Another study found that “Creatine supplementation enhanced measures of memory performance in healthy individuals, especially in older adults (66–76 years).”[ref]
Creatine and the Methylation Cycle:
The methylation cycle is a cellular process for producing methyl groups (a carbon + 3 hydrogen atoms) for use in many types of biochemical reactions. Both folate and choline are key contributors of methyl groups in the methylation cycle.
I mentioned above that one step in creatine biosynthesis includes a methyl group. A significant portion of the body’s methyl groups – about 40% – is dedicated to producing creatine.[ref]
When methyl groups are low, homocysteine levels will often be elevated. High homocysteine is linked to an elevated risk of heart problems.
Related article: Homocysteine, heart health, and more
A placebo-controlled clinical trial involving individuals engaged in resistance training showed that creatine supplementation over eight weeks reduced homocysteine levels. The study used an initial dose of 25 g/d of creatine for the first five days, followed by 5 g/day for the rest of the trial.[ref]
Methyl groups also play a role in detoxification processes, including arsenic detoxification. A study found that in people with suboptimal intake of choline or folate, supplementing with creatine or folic acid helps aid the detox reaction for arsenic.[ref]
Creatine in adipose (fat) tissue:
In fat cells (adipose tissue), creatine is important in thermogenic respiration. Loss of creatine can decrease whole-body energy expenditure.[ref]
Brown or beige fat is the type of fat that creates heat in the body, especially in babies. Brown fat is darker in color than white adipose tissue (white fat) because it contains a huge number of mitochondria cranking out heat as a metabolic waste product.
Exposure to cold can trigger brown fat to produce more energy. It is essential in infants who are too young to shiver. The brown fat helps them to maintain their temperature.
In animal studies, creatine has been shown to enhance energy production when ADP is limited. When researchers limit creatine levels, the cells try to compensate by increasing the enzymes to produce more creatine. Animals lacking the creatine kinase enzyme had increased body weight and elevated fasting blood glucose.[ref][ref] The research here is new and evolving, but it looks like creatine plays a role in adaptation to cold, energy expenditure, and metabolic health.
Sarcopenia and creatine
Sarcopenia is the loss of muscle mass, causing decreased strength in aging or chronic disease.
It is tempting to think creatine could be used to stop the aging effect on muscles, but research shows it isn’t quite that easy.
Studies in older adults show that creatine supplementation alone has little effect on muscle function or mass. But… when creatine supplementation is added to weight training, the results show that it enhances the muscle’s response to training, potentially increasing capacity for higher intensity exercise and improving the muscle’s response post-exercise.[ref]
Thus, one way that creatine may be beneficial in older adults is by increasing their capacity for exercising a little longer or lifting a little more weight. Even minor increases in exercise capacity can be important in older adults, and increasing muscle mass or grip strength can help with stability and independence.[ref]
What happens if you don’t get creatine in your diet?
While creatine can be synthesized in the body, getting additional creatine from foods may prevent problems as you age or in times of physical stress.
Low dietary creatine is associated with negative health outcomes in aging:
A study of people over age 65 found that getting less than 1g of creatine via diet each day resulted in more than double the risk of angina (chest pain) and 2.5x the risk of liver problems.
The authors of the study concluded: “The considerable shortage of dietary creatine is associated with an increased risk of heart and liver conditions, which calls for public measures that foster diets rich in creatine-containing foods, and additional research to investigate the role of creatine in age-related diseases.”[ref]
Another study found that getting over 0.95g of creatine in foods daily was protective against cognitive decline in older adults.[ref]
Clinical trials using creatine supplements:
Creatine supplements have been very well studied, with thousands of clinical trials, and looking at the trial results can give us a picture of when and where creatine supplementation is useful.
Here are just a few of the clinical trials:
| Population/Condition | Dose/Protocol | Observed Effect |
|---|---|---|
| Healthy adults (exercise) | 3 g/day | Faster recovery after muscle damage |
| Older adults (50–71 yrs) | 0.1 g/kg/day | Increased lean mass, decreased fat |
| Vegetarians | Various | Greater strength and lean mass gains |
| Hypoxic conditions | 7 days pre-exposure | Improved cognitive function |
| Alzheimer’s patients | 20 g/day | Positive cognitive results |
| Menopausal women (osteopenia) | 3 g/day | No significant bone health improvement |
| Fibromyalgia patients | 5 g/day | Increased strength, no pain/QOL improvement |
Here’s the details on those studies:
- A study from 2024 found that creatine monohydrate mediated accelerated recovery after exercise-induced muscular damage (exercise). Study participants used 3g/day of creatine.[ref] A 2025 study also showed accelerated recovery and prevented fatigue in trained athletes.[ref]
- A double-blind, placebo-controlled safety trial using 0.3g/kg of creatine per day in men found: “creatine monohydrate supplementation is safe for health and no detrimental effects on different organs and physiological systems were observed in our cohort of volunteers.”[ref]
- In healthy older adults (aged 50-71), creatine before resistance training increased lean muscle mass and decreased fat mass. The trial ran for 32 weeks and used 0.1g/kg of creatine, compared to a placebo.[ref]
- Vegetarians have lower creatine levels, on average. A study of supplemental creatine showed vegetarians had even greater increases in bench-press strength, lean tissue, and other biomarkers than did non-vegetarians. (Both groups on creatine had better results from resistance training than the vegetarian and non-vegetarian placebo groups.[ref]
- Creatine supplementation helped both men and women increase peak power in bench presses and back squats.[ref]
- Creatine plus electrolytes increased sprint cycling times in a double-blind, randomized control study.[ref]
- Under hypoxic (low oxygen) conditions, creatine helps with cognitive function. The study included 15 healthy adults who took creatine for seven days before the 90-minute hypoxia session.[ref]
- A pilot study involving Alzheimer’s patients showed positive results using 20g/day of creatine.[ref]
Negative study results are also interesting:
- Creatine supplementation (3 g/d) did not significantly improve bone health in menopausal women with osteopenia.[ref]
- In fibromyalgia patients, creatine supplementation increased muscle strength, but it didn’t reduce pain or improve quality of life.[ref]
Creatine for post-viral fatigue syndrome and Long Covid:
Post-viral fatigue syndrome is just what it sounds like – overwhelming fatigue that doesn’t end after you’ve gotten over a viral infection. It can refer to long covid or chronic fatigue syndrome (ME/CFS).
In people with post-viral fatigue syndrome (PVFS), muscle fatigue is reached much more rapidly than normal. It is thought that PVFS perturbs energy metabolism in the muscles. Research shows patients with chronic fatigue have reduced levels of hippocampal creatine, also. While there is “not enough evidence to unequivocally endorse supplemental creatine for PVFS”, researchers do think it is possibly effective, as well as being low-risk and inexpensive.[ref]
In long Covid patients, an 8-week trial of creatine, creatine + glucose, or glucose alone as the placebo, showed that creatine+glucose had a large effect on decreasing body aches, headaches, and brain fog. The participants received 8 g of creatine monohydrate and 3 g of glucose per day. [ref]
Creatine for cancer prevention:
A number of studies have investigated the question of how creatine interacts with cancer. One question for any supplement that increases energy or growth is whether it can also fuel cancer growth.
Let’s take a look at some of the recent studies on creatine and cancer. If you are under the care of an oncologist, talk with them before starting any supplements.
Studies showing creatine can help protect against cancer:
- A 2026 study in iScience showed that creatine supplementation enhances dendritic cell activation and suppresses tumor growth in an animal model of melanoma. Dendritic cells are a type of immune cell that patrols the body for abnormal cells, such as tumor cells, and then presents the tumor cell fragments to activate naive T cells. So, improving dendritic cell activation is important in how the body prevents cancer, but it is also an active field of research in improving cancer immunotherapy.[ref]
- T cells are the primary way the body fights cancer, and animal studies show that a lack of creatine causes CD8+ T cells to lose energy and become unable to kill cancer cells. Supplementing with creatine (in animals) promotes T cells to better fight cancer and suppresses tumor growth.[ref]
- A study involving data from over 7,000 people found that a higher dietary creatine intake is associated with a lower relative risk of cancer.[ref]
Clinical trials using creatine supplements in cancer patients:
A meta-analysis of clinical trials involving cancer patients taking supplemental creatine showed that there were no safety issues, but there were also no significant benefits found for muscle strength or lean mass compared to placebo.[ref]
Studies on how cancer cells can utilize creatine for energy under certain conditions:
- A cell-line study showed that colon cancer cells can use phosphocreatine through the creatine shuttle pathway as an energy production mechanism.[ref]
- In mice with cancer that has metastasized, the GATM enzyme for creatine synthesis is upregulated, and de novo synthesis of creatine is thought to increase cancer metastasis.[ref]
- In liver cancer metastasis, the GATM enzyme and creatine synthesis is also upregulated.[ref]
Big picture for creatine and cancer:
Overall, the research on creatine and cancer shows that it is dependent on context. Studies clearly show that creatine is beneficial for immune support in the prevention of cancer. However, for someone with active cancer, that picture is no longer as clear, with the animal studies showing that creatine may increase metastasis risk in certain types of cancer. As always, talk with your doctor if you have questions about what is right for you.
Creatine Synthesis Genotype Report
Access this content:
An active subscription is required to access this content.
Lifehacks:
The estimated daily requirement for creatine for an adult male weighing 70kg (154 lbs) is about 2g. Most people get about half their daily creatine from their diet, with the other half synthesized from arginine plus glycine.[ref]
Foods high in creatine
Animal proteins:
- One pound of beef contains up to 5 grams of creatine. (Note that one pound is a lot of meat)
- Fish is also an excellent source of creatine, with about 4.5 grams in one pound of salmon.[ref]
When to consider creatine supplements:
- If you aren’t eating animal-based protein-containing creatine, you may want to consider supplementing, especially if you are concerned about muscle mass or sarcopenia. Vegetarians, for example, usually have lower plasma and muscle levels of creatine.[ref]
- Creatine is synthesized from the amino acids arginine and glycine. You may also want to consider supplemental creatine if you don’t get enough glycine and arginine in your diet.
- You may also want to consider supplemental creatine if you have any genetic variants related to lower creatine production.
Let’s dig into the research on creatine supplements – how much, how often, and how it is absorbed:
Safety and Dosing of Creatine Monohydrate:
Creatine monohydrate comes as a flavorless powder and easily mixes into water or a drink, or you can get it in flavored drink mixes.
What does supplemental creatine do?
There is quite a bit of research showing that supplemental creatine is beneficial in exercise and in strength training. It isn’t a miracle supplement that will make you look like Arnold Schwarzenegger, but hundreds of research studies show it gives a bit of a muscle-building and muscle-repair boost.
You may have read that creatine supplements can cause weight gain. Researchers think the initial weight gain sometimes noticed with higher doses comes from increased water weight and not from increased body fat.[ref]
Safety and quality:
As with all supplements, choose a high-quality brand to avoid contaminants. Labdoor is one company independently testing the purity of different creatine brands. ConsumerLab.com is another company that does independent testing of supplements and reports on their quality and cost. All of the supplement brands that they tested contained creatine within the range of the amount listed on their labels. They also tested to make sure that the supplemental creatine didn’t contain an unacceptable amount of creatinine or dicyadiamide. On ConsumerLab.com, brands that passed their testing included BulkSupplements (top pick), GNC, Legion, Optimum Nutrition, PEScience, Thorne, Universal Creatine Chews (top pick), and Old School Vintage Build.[ref]
Dosing:
Studies often use a large loading dose of 20g/day for 5-7 days, followed by chronic dosing of 3-5g/day with no safety issues.
Safety assessment studies show creatine is safe at doses of up to 5g/day for long-term supplementation in healthy adults.[ref]
If you have health concerns, especially kidney disease, you should talk with your doctor to be sure that creatine is safe for you. The studies on healthy people show creatine to be safe, but there are a few case studies with chronic kidney disease patients having problems with supplemental creatine.[ref]
Side effects, tips, and cautions with creatine supplements:
Anecdotal reports on the web mention gastrointestinal distress when using higher doses too quickly. If you aren’t using creatine for bodybuilding and find it gives you intestinal issues, try going with the lower doses to start with.
Dissolving it well:
Creatine doesn’t dissolve all that well in cold water, so if you have gastrointestinal side effects, it could be due to it not dissolving before it hits the intestines. Try stirring it into warm water, tea, or coffee, and go with divided doses, if needed. For drinks that come prepackaged with creatine, a study showed that keeping it in the refrigerator made re-crystalization happen within a week.[ref]
Precaution: asthma
If you have asthma, talk with your doctor before supplementing with creatine. Studies in mice show that creatine may exacerbate airway sensitivity, which theoretically could make asthma worse.[ref]
Creatine Gummies Vs Creatine Monohydrate Powder
ConsumerLab.com tested six popular creatine gummy brands and found that four contained “virtually” no creatine. The other two contained high levels of creatinine, a breakdown product of creatine. Of the creatine powders they tested, all contained the amounts of creatine they claimed and passed the other tests ConsumerLab requires. [ref] Thus, a powdered form of creatine supplement may be a much better option than a gummy (or look for third-party testing for the gummy options to know the creatine levels).
What has creatine been studied for?
Stopping exercise-induced muscle damage:
A huge meta-analysis of 20 different studies showed that creatine monohydrate lowered levels of muscle damage after acute training.[ref]
Improving muscle mass in weight training:
Quite a few clinical trials show that creatine supplements can help to improve muscle mass while decreasing damage.[ref][ref][ref]
Mood disorders:
Clinical trials show that creatine may help with depression caused by a lack of brain energy or oxidative stress.[ref] In people with bipolar disorder, 6g/day of creatine was trialed against a placebo. The treatment group had better verbal fluency test scores after six weeks.[ref] Other studies also showed mild efficacy for creatine in bipolar disorder.[ref]
Cognitive function in young adults: Not a big benefit
Clinical trial results don’t show much of an effect of creatine supplementation on cognitive processing speed in healthy young adults.[ref] One trial did show a small beneficial effect in healthy young adults, with half of the participants being vegetarians.[ref]
Cognitive function in older adults: Beneficial
A clinical trial using 5g four times a day for a week showed a significant improvement in cognitive function test scores.[ref]
The opposite results for healthy younger people vs. older adults make sense to me. Creatine seems to be useful for brain energy production when the brain is under stress (e.g., sleep deprivation or brain injury). It may also be helpful in dementia or chronic neurological stressors.[ref] But for someone young, healthy, and getting enough sleep, the brain likely has enough ATP and enough creatine on hand to meet its needs without supplementing.
Creatine Stacks:
Often, you’ll see creatine combined with other supplements with marketing claims that it is superior to creatine alone. The following ‘stacks’ have clinical trial data:
- Sodium bicarbonate:
A trial of creatine vs. creatine + sodium bicarbonate vs. placebo found that average power increased more with creatine + sodium bicarbonate. The study was done on taekwondo athletes using 20g of creatine plus 0.5g/kg of sodium bicarbonate.[ref] - Guanidinoacetic acid (GAA):
Creatine + GAA was shown to be a little bit better at increasing creatine levels in skeletal muscle and gray matter in the brain.[ref] However, some studies point to GAA increasing oxidative stress in the brain.[ref]
Doses for cognitive function:
The optimal dose of creatine likely depends on someone’s underlying brain health. If you are on medications and have any questions about creatine or other dietary supplements, talk with your doctor or pharmacist before supplementing.
A study on brain creatine levels showed that 8g/day for 16 weeks increased levels by 7-13%. Another study showed 10g/day for six months increased brain creatine levels by 8%. A loading dose of 20g/day for five days, followed by 2g/day for seven days, also increased brain creatine levels by 8%.[ref]
Absorption and metabolism of creatine:
Creatine is absorbed in the intestines. Taking supplemental creatine at the same time as carbohydrates enhances muscle uptake of creatine. But… a high sugar concentration can slow the absorption of creatine.[ref]
Thus, you may want to add your creatine supplement along with a meal with some carbs in it.
Creatine and phosphocreatine in muscles degrade into creatinine. The kidneys can also clear out creatine in the urine.
The half-life of supplemental creatine in a healthy male adult is between 3 and 4 hours.[ref] This means that about half of the creatine is metabolized, or used, in 3-4 hours. It doesn’t seem to be as simple as you’ve used up half the creatine in 3-4 hours and thus get a benefit from taking more. Your creatine levels can depend on how much is being used in the muscles and brain, as well as how much is already available or stored in the muscles. The whole idea of using a high dose for a few days is to load the muscle cells with creatine and then use a lower dose for steady-state maintenance.
Creatine with MTHFR C677T: Boosting methylation pathway function
Because creatine production uses methyl groups, creatine supplementation may be especially relevant for people with MTHFR variants, since it can help reduce one source of methylation demand. Creatine synthesis is linked to methylation because one of the final steps requires methyl groups. When creatine is supplied through food or supplements, endogenous creatine production can decrease, which may “spare” methyl groups and potentially ease the load on the methylation cycle.
Methyl groups are also used for remethylating homocysteine, and homocysteine levels can rise when there are insufficient methyl groups available. Clinical trials show that supplemental creatine can lower homocysteine levels in healthy people with good kidney function. This directly ties creatine supplementation to sparing methyl groups for homocysteine remethylation.[ref][ref][ref]
For people with MTHFR variants, this connection may matter even more because the methylation cycle can already be less efficient. In that context, creatine supplementation may help reduce the body’s need to spend methyl groups on making creatine, leaving more methylation capacity available for other functions. If you have the MTHFR C677T variant (below), you may find benefit in increasing creatine either through supplemental creatine or creatine-rich foods. This is also a good way to get around supplementing with methylfolate, which may be important if you also have slow COMT function.
Access this content:
An active subscription is required to access this content.
Related B Vitamins and Methylation
- MTHFR (folate)
- Choline (PEMT)
- Vitamin B12 (MTR, MTRR)
- Riboflavin (cofactor in methylation)
- Vitamin B6
- Thiamine (Vitamin B1)
- Vitamin B5 (Pantothenic acid)
- COMT (Affects response to methylated vitamins)
Related Articles and Topics:
References:
Salem, Atef, et al. “Short-Term Creatine Supplementation Enhances Strength, Reduces Fatigue, and Accelerates Recovery in Resistance-Trained Athletes: A Double-Blind, Randomized, Crossover Trial.” Journal of the International Society of Sports Nutrition, vol. 22, no. sup1, Sept. 2025, p. 2617283. PubMed, https://doi.org/10.1080/15502783.2026.2617283.
Alessandrì, Maria Grazia, et al. “Increased Creatine Demand during Pregnancy in Arginine: Glycine Amidino-Transferase Deficiency: A Case Report.” BMC Pregnancy and Childbirth, vol. 20, no. 1, Sept. 2020, p. 506. PubMed, https://doi.org/10.1186/s12884-020-03192-4.
Almeida, Douglas, et al. “Creatine Supplementation Improves Performance, but Is It Safe? Double-Blind Placebo-Controlled Study.” The Journal of Sports Medicine and Physical Fitness, vol. 60, no. 7, July 2020, pp. 1034–39. PubMed, https://doi.org/10.23736/S0022-4707.20.10437-7.
Alves, Christiano R. R., et al. “Creatine Supplementation in Fibromyalgia: A Randomized, Double-Blind, Placebo-Controlled Trial.” Arthritis Care & Research, vol. 65, no. 9, Sept. 2013, pp. 1449–59. PubMed, https://doi.org/10.1002/acr.22020.
Assanangkornchai, N., et al. “Characteristics of Trauma Patients with Creatine Kinase Elevation.” Critical Care, vol. 19, no. Suppl 1, 2015, p. P282. PubMed Central, https://doi.org/10.1186/cc14362.
Balberova, Olga V., et al. “Candidate Genes of Regulation of Skeletal Muscle Energy Metabolism in Athletes.” Genes, vol. 12, no. 11, Oct. 2021, p. 1682. PubMed Central, https://doi.org/10.3390/genes12111682.
Bereket-Yücel, S. “Creatine Supplementation Alters Homocysteine Level in Resistance Trained Men.” The Journal of Sports Medicine and Physical Fitness, vol. 55, no. 4, Apr. 2015, pp. 313–19.
Bozack, Anne K., et al. “Betaine and Choline Status Modify the Effects of Folic Acid and Creatine Supplementation on Arsenic Methylation in a Randomized Controlled Trial of Bangladeshi Adults.” European Journal of Nutrition, vol. 60, no. 4, June 2021, pp. 1921–34. PubMed, https://doi.org/10.1007/s00394-020-02377-z.
Brosnan, John T., et al. “The Metabolic Burden of Creatine Synthesis.” Amino Acids, vol. 40, no. 5, May 2011, pp. 1325–31. PubMed, https://doi.org/10.1007/s00726-011-0853-y.
Brosnan, Margaret E., and John T. Brosnan. “The Role of Dietary Creatine.” Amino Acids, vol. 48, no. 8, Aug. 2016, pp. 1785–91. PubMed, https://doi.org/10.1007/s00726-016-2188-1.
Burke, Darren G., et al. “Effect of Creatine and Weight Training on Muscle Creatine and Performance in Vegetarians.” Medicine and Science in Sports and Exercise, vol. 35, no. 11, Nov. 2003, pp. 1946–55. PubMed, https://doi.org/10.1249/01.MSS.0000093614.17517.79.
Cabaniss, C. Daniel. “Creatine Kinase.” Clinical Methods: The History, Physical, and Laboratory Examinations, edited by H. Kenneth Walker et al., 3rd ed., Butterworths, 1990. PubMed, http://www.ncbi.nlm.nih.gov/books/NBK352/.
Candow, Darren G., et al. “Strategic Creatine Supplementation and Resistance Training in Healthy Older Adults.” Applied Physiology, Nutrition, and Metabolism = Physiologie Appliquee, Nutrition Et Metabolisme, vol. 40, no. 7, July 2015, pp. 689–94. PubMed, https://doi.org/10.1139/apnm-2014-0498.
Chiou, W. L., and F. H. Hsu. “Pharmacokinetics of Creatinine in Man and Its Implications in the Monitoring of Renal Function and in Dosage Regimen Modifications in Patients with Renal Insufficiency.” Journal of Clinical Pharmacology, vol. 15, no. 5–6, June 1975, pp. 427–34. PubMed, https://doi.org/10.1002/j.1552-4604.1975.tb02364.x.
Crisafulli, Daniel L., et al. “Creatine-Electrolyte Supplementation Improves Repeated Sprint Cycling Performance: A Double Blind Randomized Control Study.” Journal of the International Society of Sports Nutrition, vol. 15, 2018, p. 21. PubMed, https://doi.org/10.1186/s12970-018-0226-y.
De Moura Leite, Luciana, et al. “Creatine Supplementation in Patients With Cancer: A Systematic Review and Meta‐Analysis.” JCSM Communications, vol. 9, no. 1, Jan. 2026, p. e70044. DOI.org (Crossref), https://doi.org/10.1002/rco2.70044.
Dolan, Eimear, et al. “Muscular Atrophy and Sarcopenia in the Elderly: Is There a Role for Creatine Supplementation?” Biomolecules, vol. 9, no. 11, Oct. 2019, p. E642. PubMed, https://doi.org/10.3390/biom9110642.
Doma, Kenji, et al. “The Paradoxical Effect of Creatine Monohydrate on Muscle Damage Markers: A Systematic Review and Meta-Analysis.” Sports Medicine, vol. 52, no. 7, July 2022, pp. 1623–45. Springer Link, https://doi.org/10.1007/s40279-022-01640-z.
Dubé, Marie-Pierre, et al. “CKM and LILRB5 Are Associated with Serum Levels of Creatine Kinase.” Circulation. Cardiovascular Genetics, vol. 7, no. 6, Dec. 2014, pp. 880–86. PubMed, https://doi.org/10.1161/CIRCGENETICS.113.000395.
Fernández-Torres, Javier, et al. “Ancestral Contribution of the Muscle-Specific Creatine Kinase (CKM) Polymorphism Rs4884 in the Knee Osteoarthritis Risk: A Preliminary Study.” Clinical Rheumatology, vol. 40, no. 1, Jan. 2021, pp. 279–85. PubMed, https://doi.org/10.1007/s10067-020-05238-6.
Forbes, Scott C., et al. “Effects of Creatine Supplementation on Brain Function and Health.” Nutrients, vol. 14, no. 5, Feb. 2022, p. 921. PubMed Central, https://doi.org/10.3390/nu14050921.
George, Michael D., et al. “Creatine Kinase in the U.S. Population: Impact of Demographics, Comorbidities, and Body Composition on the Normal Range.” Medicine, vol. 95, no. 33, Aug. 2016, p. e4344. PubMed, https://doi.org/10.1097/MD.0000000000004344.
Horino, Masato, et al. “The Role of Thermogenic Fat Tissue in Energy Consumption.” Current Issues in Molecular Biology, vol. 44, no. 7, July 2022, pp. 3166–79. PubMed Central, https://doi.org/10.3390/cimb44070219.
Hummer, Erik, et al. “Creatine Electrolyte Supplement Improves Anaerobic Power and Strength: A Randomized Double-Blind Control Study.” Journal of the International Society of Sports Nutrition, vol. 16, no. 1, May 2019, p. 24. PubMed, https://doi.org/10.1186/s12970-019-0291-x.
Kang, Elliot, et al. “Creatine Uptake Promotes Dendritic Cell Activation and Enhances Antitumor Immunity.” iScience, vol. 29, no. 4, Apr. 2026, p. 115436. DOI.org (Crossref), https://doi.org/10.1016/j.isci.2026.115436.
Kazak, Lawrence, et al. “A Creatine-Driven Substrate Cycle Enhances Energy Expenditure and Thermogenesis in Beige Fat.” Cell, vol. 163, no. 3, Oct. 2015, pp. 643–55. PubMed Central, https://doi.org/10.1016/j.cell.2015.09.035.
Kazak, Lawrence, and Paul Cohen. “Creatine Metabolism: Energy Homeostasis, Immunity and Cancer Biology.” Nature Reviews. Endocrinology, vol. 16, no. 8, Aug. 2020, pp. 421–36. PubMed, https://doi.org/10.1038/s41574-020-0365-5.
Kobayashi, Yoshio, et al. “Effect of a Marathon Run on Serum Lipoproteins, Creatine Kinase, and Lactate Dehydrogenase in Recreational Runners.” Research Quarterly for Exercise and Sport, vol. 76, no. 4, Dec. 2005, pp. 450–55. PubMed, https://doi.org/10.1080/02701367.2005.10599318.
Mangravite, Lara M., et al. “A Statin-Dependent QTL for GATM Expression Is Associated with Statin-Induced Myopathy.” Nature, vol. 502, no. 7471, Oct. 2013, pp. 377–80. PubMed Central, https://doi.org/10.1038/nature12508.
McMorris, Terry, et al. “Creatine Supplementation and Cognitive Performance in Elderly Individuals.” Neuropsychology, Development, and Cognition. Section B, Aging, Neuropsychology and Cognition, vol. 14, no. 5, Sept. 2007, pp. 517–28. PubMed, https://doi.org/10.1080/13825580600788100.
NM_001482.3(GATM):C.446G>A (p.Trp149Ter) AND Arginine:Glycine Amidinotransferase Deficiency – ClinVar – NCBI. https://www.ncbi.nlm.nih.gov/clinvar/112859991/. Accessed 15 Nov. 2022.
Ostojic, Sergej M. “Diagnostic and Pharmacological Potency of Creatine in Post-Viral Fatigue Syndrome.” Nutrients, vol. 13, no. 2, Feb. 2021, p. 503. PubMed Central, https://doi.org/10.3390/nu13020503.
—. “Dietary Creatine and Cognitive Function in U.S. Adults Aged 60 Years and Over.” Aging Clinical and Experimental Research, vol. 33, no. 12, Dec. 2021, pp. 3269–74. PubMed, https://doi.org/10.1007/s40520-021-01857-4.
—. “Dietary Intake of Creatine and Risk of Medical Conditions in U.S. Older Men and Women: Data from the 2017-2018 National Health and Nutrition Examination Survey.” Food Science & Nutrition, vol. 9, no. 10, Oct. 2021, pp. 5746–54. PubMed, https://doi.org/10.1002/fsn3.2543.
Rawson, Eric S., et al. “Creatine Supplementation Does Not Improve Cognitive Function in Young Adults.” Physiology & Behavior, vol. 95, no. 1–2, Sept. 2008, pp. 130–34. PubMed, https://doi.org/10.1016/j.physbeh.2008.05.009.
Roschel, Hamilton, et al. “Creatine Supplementation and Brain Health.” Nutrients, vol. 13, no. 2, Feb. 2021, p. 586. PubMed, https://doi.org/10.3390/nu13020586.
Sales, Lucas Peixoto, et al. “Creatine Supplementation (3 g/d) and Bone Health in Older Women: A 2-Year, Randomized, Placebo-Controlled Trial.” The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences, vol. 75, no. 5, Apr. 2020, pp. 931–38. PubMed, https://doi.org/10.1093/gerona/glz162.
Sarshin, Amir, et al. “Short-Term Co-Ingestion of Creatine and Sodium Bicarbonate Improves Anaerobic Performance in Trained Taekwondo Athletes.” Journal of the International Society of Sports Nutrition, vol. 18, no. 1, Jan. 2021, p. 10. PubMed, https://doi.org/10.1186/s12970-021-00407-7.
Schlattner, Uwe, et al. “Mitochondrial Creatine Kinase in Human Health and Disease.” Biochimica Et Biophysica Acta, vol. 1762, no. 2, Feb. 2006, pp. 164–80. PubMed, https://doi.org/10.1016/j.bbadis.2005.09.004.
Semeredi, Sasa, et al. “Guanidinoacetic Acid with Creatine Compared with Creatine Alone for Tissue Creatine Content, Hyperhomocysteinemia, and Exercise Performance: A Randomized, Double-Blind Superiority Trial.” Nutrition (Burbank, Los Angeles County, Calif.), vol. 57, Jan. 2019, pp. 162–66. PubMed, https://doi.org/10.1016/j.nut.2018.04.009.
Shao, Andrew, and John N. Hathcock. “Risk Assessment for Creatine Monohydrate.” Regulatory Toxicology and Pharmacology: RTP, vol. 45, no. 3, Aug. 2006, pp. 242–51. PubMed, https://doi.org/10.1016/j.yrtph.2006.05.005.
Taylor, Beth A., et al. “Increased Creatine Kinase with Statin Treatment May Identify Statin-Associated Muscle Symptoms.” International Journal of Cardiology, vol. 209, Apr. 2016, pp. 12–13. PubMed Central, https://doi.org/10.1016/j.ijcard.2016.02.028.
Toniolo, Ricardo Alexandre, Michelle Silva, et al. “A Randomized, Double-Blind, Placebo-Controlled, Proof-of-Concept Trial of Creatine Monohydrate as Adjunctive Treatment for Bipolar Depression.” Journal of Neural Transmission (Vienna, Austria: 1996), vol. 125, no. 2, Feb. 2018, pp. 247–57. PubMed, https://doi.org/10.1007/s00702-017-1817-5.
Toniolo, Ricardo Alexandre, Francy de Brito Ferreira Fernandes, et al. “Cognitive Effects of Creatine Monohydrate Adjunctive Therapy in Patients with Bipolar Depression: Results from a Randomized, Double-Blind, Placebo-Controlled Trial.” Journal of Affective Disorders, vol. 224, Dec. 2017, pp. 69–75. PubMed, https://doi.org/10.1016/j.jad.2016.11.029.
Turner, Clare E., et al. “Creatine Supplementation Enhances Corticomotor Excitability and Cognitive Performance during Oxygen Deprivation.” The Journal of Neuroscience: The Official Journal of the Society for Neuroscience, vol. 35, no. 4, Jan. 2015, pp. 1773–80. PubMed, https://doi.org/10.1523/JNEUROSCI.3113-14.2015.
Wallace, B., et al. “Common Creatine Kinase Gene Mutation Results in Falsely Reassuring CK Levels in Muscle Disorders.” QJM: An International Journal of Medicine, vol. 109, no. 6, June 2016, pp. 413–14. PubMed Central, https://doi.org/10.1093/qjmed/hcv215.
Youn, Bo-Young, et al. “Genetic Basis of Elite Combat Sports Athletes: A Systematic Review.” Biology of Sport, vol. 38, no. 4, Oct. 2021, pp. 667–75. PubMed Central, https://doi.org/10.5114/biolsport.2022.102864.
Zhang, Liwen, et al. “Creatine Promotes Cancer Metastasis through Activation of Smad2/3.” Cell Metabolism, vol. 33, no. 6, June 2021, pp. 1111-1123.e4. DOI.org (Crossref), https://doi.org/10.1016/j.cmet.2021.03.009.