Key takeaways:
- Plasminogen Activator Inhibitor (PAI-1) is an enzyme that helps regulate how quickly the body breaks down blood clots and is also involved in fibrosis and tissue remodeling.
- Higher PAI-1 levels are associated with an increased relative risk of heart attack, stroke, blood clots, tissue fibrosis, miscarriage, senescence in aging, and metabolic problems.
- Variants in the SERPINE1 gene can influence your baseline PAI-1 levels, affecting clotting and fibrosis risk.
- Lifestyle, diet, and natural compounds may help to lower elevated PAI-1 levels.
Members will see their genotype report below, plus additional solutions in the Lifehacks section. Consider joining today.
What is Plasminogen Activator Inhibitor-1 (PAI-1)?
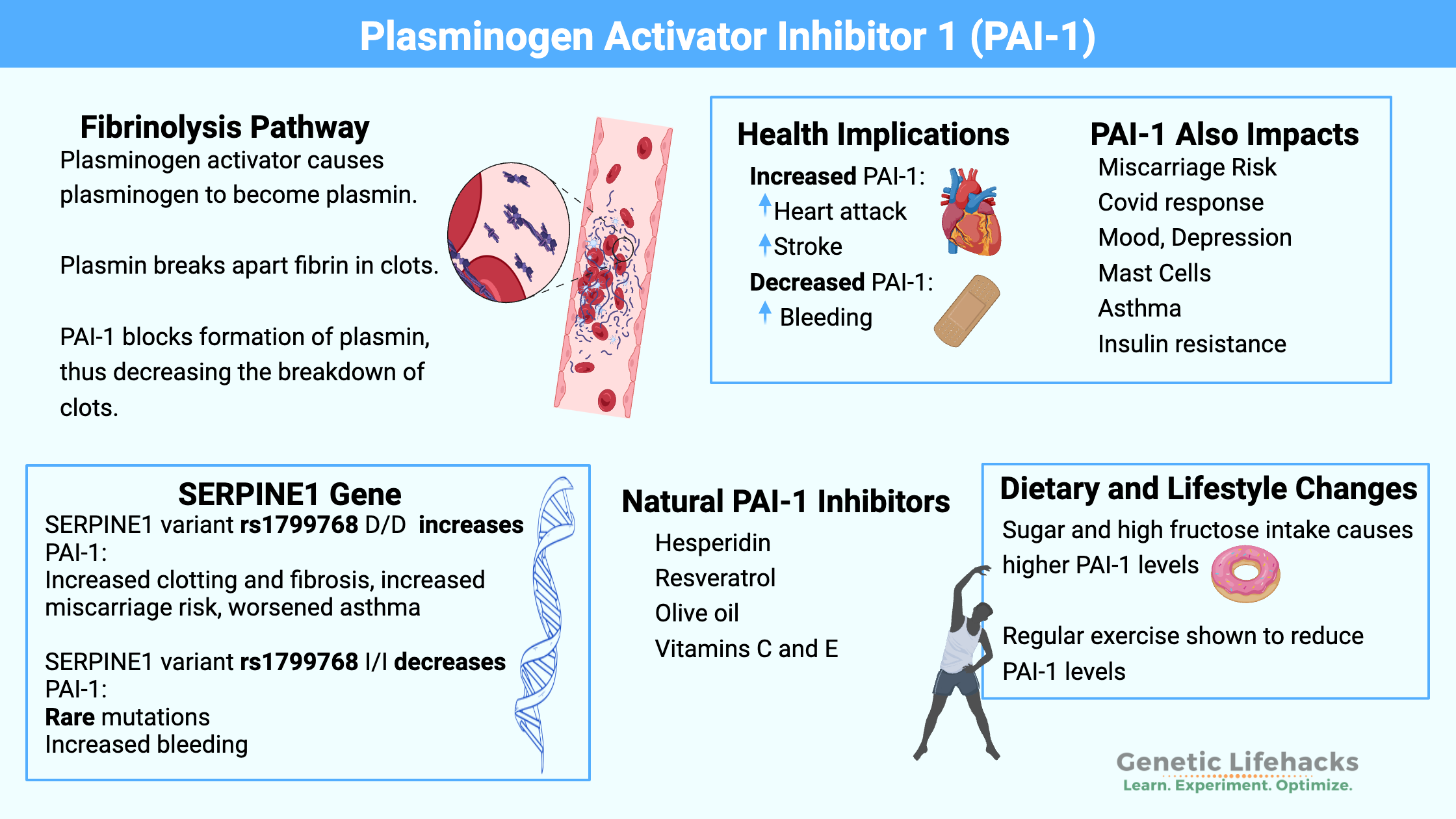
PAI-1, or plasminogen activator inhibitor-1, is a protein that helps keep clot breakdown under control. It inhibits tPA and uPA, which are involved in fibrinolysis, the process of dissolving clots and fibrosis. Because of that, PAI-1 sits at the intersection of clotting, fibrosis, and tissue repair, but it also interacts with pregnancy, metabolic health, and longevity.
Protease inhibitor: PAI-1 is classified as a serine protease inhibitor. Proteases are enzymes that break apart peptide bonds in proteins. Serine is an amino acid that is part of this type of protease enzyme. In the body, protease enzymes have to be kept in check – neutralized – by protease inhibitors so that the proteases do not overreact and damage healthy tissues
PAI-1 acts as an inhibitor for two proteins:
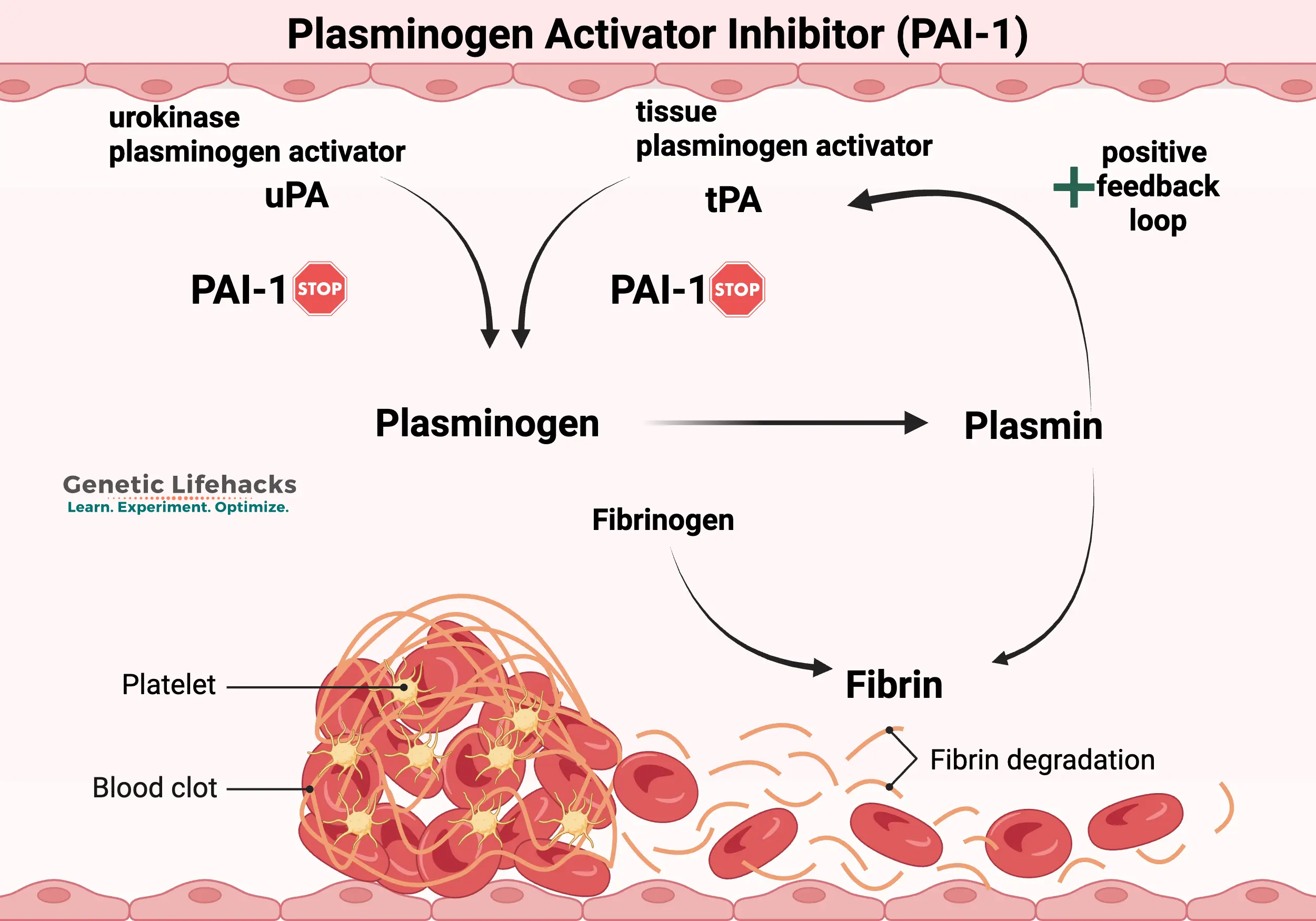
- PAI-1 inhibits the action of tissue-type plasminogen activator (tPA). Tissue-type plasminogen activator is involved in degrading the fibrin network in clots through a process called fibrinolysis. In this way, tPA causes the breakdown of clots. Inhibiting tPA with PAI-1 therefore prevents too much fibrinolysis (too much clot breakdown). Tissue plasminogen activator is synthesized by endothelial cells that line blood vessels.
- PAI-1 also inhibits urokinase plasminogen activator (uPA), which is the enzyme that cleaves plasminogen to form plasmin.[ref] uPA is synthesized in monocytes and macrophages, which are immune system cells. It is also synthesized in urinary epithelial cells.
By inhibiting the activation of plasminogen to plasmin, PAI-1 is part of the continual balancing act of breaking down and forming the fibrin network in clots.
In a nutshell, PAI-1 inhibits fibrinolysis, the process of breaking down clots.[ref] It is key to the delicate balance in clotting:
- Too little PAI-1 can increase the risk of hemorrhaging or excessive bleeding
- Too much PAI-1 can increase the risk of inappropriate blood clot formation
| Question | Simple answer |
|---|---|
| What is PAI‑1? | A protein (serine protease inhibitor) that slows down the breakdown of blood clots and fibrin. |
| Why does it matter? | Too much PAI‑1 means more clotting and fibrosis; too little means higher bleeding risk. |
| Where is it made? | Mainly in endothelial cells, liver, fat tissue, and some immune and brain cells. |
| What raises PAI‑1? | Genetics, aging, stress and cortisol, insulin resistance/NAFLD, obesity, inflammation, and some cancers. |
| What can high PAI‑1 contribute to? | Heart attack, stroke, venous clots, fibrosis (lung, heart, uterus), pregnancy complications, and possibly mood and cognitive changes. |
| Can genes affect my PAI‑1 level? | Yes, common SERPINE1 variants (including the 4G/5G promoter polymorphism) can shift baseline PAI‑1 up or down. |
| Are there ways to lower high PAI‑1? | Lower glycemic load, address insulin resistance and fatty liver, regular exercise, and certain natural compounds (e.g., hesperidin, resveratrol, olive phenolics) show PAI‑1–modulating effects in studies. |
| Big picture | PAI‑1 sits at the intersection of clotting, fibrosis, metabolism, aging, and stress biology. |
Background science: Understanding fibrinolysis and clotting
Blood clots form in response to wounds or other inflammatory stimuli. Clots are formed from activated platelets, red blood cells, and cross-linked fibrin proteins that form a mesh. The fibrin mesh is made through a series of steps from fibrinogen, a protein that circulates in the blood.[ref]
Blood clots actively dissolve and reform in a continuous process. It is a tightly regulated balancing act between fibrin formation and fibrinolysis.
- Activation of plasminogen: Plasminogen is an inactive form of plasmin that circulates in the blood. Fibrinolysis begins when plasminogen is converted into plasmin, its active form. Tissue plasminogen activator (tPA) and urokinase plasminogen activator (uPA) are the enzymes that convert plasminogen into plasmin to break down fibrin. tPA is released from the endothelial cells in response to the initiation of the clotting process (thrombin).
- Active plasmin: Plasmin is an enzyme that cleaves fibrin into fibrin degradation products. D-dimer is one of these fibrin degradation products and is usually measured to see if someone has a clot.
- Feedback loop: In a positive feedback loop, plasmin activates tPA and uPA, leading to further activation of plasminogen to plasmin and increasing the breakdown of the clot.
- Inhibition of plasmin: This is where PAI-1 comes in – it inhibits the activation of plasminogen into plasmin and acts as a brake on the system. There is also another protein, alpha-2-antiplasmin, which can inhibit the active plasmin.
Feedback loops, regulation of the processes — when everything is in balance, the clot forms quickly, is constantly remodeled, and then dissolves away when it is no longer needed.
Too little fibrinolysis is called hypofibrinolysis. This can lead to a thrombosis (clot) that can travel to the heart or lungs and be fatal. Hypofibrinolysis can be caused by autoantibodies to tPA or uPA or by genetic variants that increase PAI-1.
Plasmin Activator Inhibitor family:
While the focus of this article is PAI-1, it’s important to note that it isn’t the only plaminogen activator inhibitor. PAI-1 is responsible for about 60% of the PA inhibitory activity in the plasma, but there are two other enzymes, PAI-2 and PAI-3, which are involved in PA inhibition under certain circumstances (pregnancy, tumors). PAI-3 is also known as protein C inhibitor and plays a role in the implantation of the fetus during early pregnancy.[ref]
Conditions associated with higher PAI-1 levels:
Higher PAI-1 levels are associated with cardiovascular disease, metabolic disease, cancer, tissue fibrosis in inflammation, neurodegenerative disease, and mood disorders.[ref]
| System / Condition | What happens with PAI‑1? | Why does it matter? |
|---|---|---|
| Heart attack, DVT, stroke | Higher PAI‑1 levels and “high‑PAI‑1” genotypes are associated with more stable clots and increased risk of myocardial infarction, venous thromboembolism, and ischemic stroke. | Higher relative risk of heart attack, leg clots, and brain clots, especially when combined with other pro‑thrombotic factors. |
| Atherosclerosis | Plaque areas often show higher local PAI‑1 expression. | May contribute to plaque progression and reduced fibrinolysis on plaque surfaces. |
| Lung and organ fibrosis | Overexpression of PAI‑1 promotes lung fibrosis and other tissue fibrosis; too little in some contexts can also dysregulate remodeling. | Can worsen scarring in lung, heart valves, and other organs. |
| Brain and mood | Elevated PAI‑1 seen in depression; both excess and deficiency affect BDNF processing and monoamine metabolism in animal models. | Links stress, mood, and cognition to PAI‑1 pathways. |
| Aging / immunosenescence | PAI‑1 rises with age and tracks with senescent cell burden; experimental inhibition reduces senescence and thrombosis in models. | Ties PAI‑1 to age‑related inflammation, clotting, and immune aging. |
| COVID‑19 and infections | Severe Covid and spike‑protein exposure are associated with high PAI‑1 and more resistant clots. | Helps explain “sticky blood” and clotting tendency in severe COVID‑19. |
| Insulin resistance & NAFLD | Insulin resistance, obesity, and fatty liver correlate with elevated PAI‑1 produced by the liver and adipose tissue. | Links metabolic syndrome and type 2 diabetes to higher clotting risk. |
| Asthma & mast cell activation | Mast cells induce endothelial PAI‑1; high‑PAI‑1 genotypes associate with worse airflow limitation. | Adds a fibrosis and remodeling dimension to asthma severity. |
| Pregnancy complications | Excess PAI‑1 in pregnancy is linked to miscarriage, preeclampsia, and gestational diabetes in some studies. | Important consideration in recurrent pregnancy loss and high‑risk pregnancies. |
| Cancer | In several tumors, PAI‑1 expression is associated with tumor progression and thrombosis risk. | Potential prognostic marker and therapeutic target in oncology. |
Let’s take a look at these in depth.
Blood clots, heart attacks, and strokes:
PAI-1 levels directly affect clotting, with higher levels increasing clotting and low levels leading to increased bleeding risk.
- Myocardial infarction: Researchers have known for three decades that certain variants in the gene that codes for PAI-1 cause an increased risk of heart attack due to blood clots. The variants increase the amount of PAI-1 that is made by the body, and so there is less degradation of the clot.[ref][ref]
- Blood clots: PAI-1 levels are often elevated in people with deep vein thrombosis (DVT).[ref][ref] Similarly, the risk of venous thromboembolism is increased with higher levels of PAI-1.[ref]
- Stroke: Ischemic strokes are caused by a blood clot in the brain that reduces blood flow to an area. Genetic variants that increase PAI-1 levels are linked to an increased risk of stroke.[ref] One drug that people who have an ischemic stroke receive is recombinant tPA to increase plasmin levels to dissolve the clot.
Atherosclerosis: Atherosclerotic plaque formation is associated with higher PAI-1 expression in the local plaque area. Not all studies agree on whether higher circulating levels of PAI-1 are involved in the development of atherosclerosis, and there are likely other factors involved.[ref]
PAI-1 and fibrosis:
Fibrosis occurs when too much extracellular matrix is deposited, such as in a scar that forms during wound healing.
While we usually think of scarring in terms of skin wounds, fibrosis can also occur when an organ is subjected to an insult or dysfunction. For example, lung fibrosis can occur due to smoking or asbestos exposure – both of which cause a little damage to the lungs.
PAI-1 comes into play here because it controls the breakdown of fibrin, which is integral to fibrosis. PAI-1 balances the formation of fibrin by uPA and tPA. Normally, when there is a wound, levels of PAI-1 are somewhat elevated to inhibit uPA and tPA and speed wound healing.[ref]
In general, if PAI-1 levels are too high, there may be excessive accumulation of extracellular matrix proteins and collagen. When PAI-1 levels are too low in the heart, spontaneous fibrosis can also occur.[ref]
- Lung fibrosis: Animal studies show that overexpression of PAI-1 causes an increase in lung fibrosis, such as in hypersensitivity pneumonitis, idiopathic pulmonary fibrosis, silicosis, and cystic fibrosis.[ref] Studies involving PAI-1 inhibitors show that they can attenuate the COPD and emphysema pathology from cigarette smoking.[ref]
- Heart valve stenosis: In a study of aortic valves undergoing replacement, researchers found that fibrosis in the valves correlated with higher levels of PAI-1 as well as higher levels of LDL.[ref]
- Endometrial fibrosis: A 2025 study showed that PAI-1 is integral to the initiation and formation of endometrial fibrosis in intrauterine adhesions, which is a cause of infertility. Inhibiting PAI-1 mitigated the endometrial fibrosis.[ref]
In the brain: PAI-1, neurotransmitters, and mood
Plasminogen activator inhibitor-1 is found in areas of the brain associated with mood (prefrontal cortex, amygdala, hippocampus) as well as in the bloodstream of the brain. Studies show that depressed patients have higher plasma levels of PAI-1. Animal studies show that chronic, unpredictable mild stress causes an increase in PAI-1 in the brain. This is just one connection between stress, cortisol, and mood changes.[ref] A 2026 study found that inhibiting PAI-1 after a few weeks of intermittent stress reduced anxiety-like behaviors and depression-like responses in animals.[ref]
It’s not as simple, though, as too much PAI-1 causes depression, since PAI-1 has multiple roles in the brain.
BDNF is a neurotrophic factor that interacts with PAI-1. The precursor form, proBDNF, is cleaved by plasminogen activator (PA) to form the mature form of BDNF. BDNF helps the brain form new synaptic connections and maintain plasticity. [ref]
Animal research shows that PAI-1 deficiency causes depressive-like behaviors. The results showed that PAI-1 plays a role in depression beyond simply inhibiting PA, which could decrease BDNF. Instead, the researchers found that a complete lack of PAI-1 impairs the metabolism of serotonin and dopamine.[ref]
Related article: BDNF, cognitive function, and mood
Neurodegenerative diseases: Alzheimer’s and Parkinson’s diseases involve tangled proteins or plaques in the brain. PAI-1 may play a role in both. In a mouse model of Alzheimer’s, inhibiting PAI-1 reduced amyloid-beta plaques.[ref]
Researchers also recently found that PAI-1 levels are higher in patients with Parkinson’s disease or Lewy body dementia. However, the research here is preliminary, and it isn’t clear whether PAI-1 and tPA are actively playing a role in the formation of alpha-synuclein.[ref]
Senescence, aging, and plasminogen activator inhibitor:
Cells are constantly being replaced in the body. For example, intestinal epithelial cells have a life span of 3-5 days. Heart muscle cells and brain cells, on the other hand, have very slow or no turnover.
Cellular senescence is the state in which a cell can no longer replicate and regenerate. Instead, it stops dividing and releases inflammatory signals so that it can be eliminated by the immune system. This is an essential check to prevent excessive growth (e.g., cancer).
As we age, the number of senescent cells overwhelms the immune system’s ability to eliminate them, leading to chronic low-grade inflammation. PAI-1 levels increase with age, and levels correlate with the number of senescent cells.[ref]
In 2006, PAI-1 was identified as a driver of cellular senescence. Research studies over the last decade show that PAI-1 is an essential part of cellular senescence and that inhibiting PAI-1 can reduce senescence in certain situations. [ref]
A 2026 study shows that PAI-1 is likely more than just a marker of aging and instead is an active part of immune system aging, interacting with senescence, chronic inflammation, and impaired immune surveillance.[ref]
Related article: Longevity Lifehacks – PAI-1 Inhibition for Longevity
Stress response: Cortisol increases PAI-1
When you are stressed, cortisol is released by the adrenal glands. The increase in cortisol causes a number of different genes to be expressed or blocked.
One effect of increased cortisol is to increase the production of tissue plasminogen activator (tPA) and PAI-1. In the brain, however, the stress response shifts so that there is an increase in PAI-1 compared to tPA. Researchers have found that this increased ratio of PAI-1 to tPA is part of the negative effect of stress on cognitive function. Blocking pro-BDNF to BDNF is thought to be part of the stress-related effects on memory and cognitive function.[ref]
PAI-1 and cancer:
PAI-1 is thought to have a function beyond its anti-fibrinolytic effects when it comes to cancer. Most research suggests it has a pro-tumor promotion role.[ref] In pancreatic tumors that express PAI-1, there is an increased risk of blood clots (venous thromboembolism).[ref]
In skin cancer, PAI-1 promotes its progression, and inhibiting PAI-1 is currently being studied as an adjunctive therapy.[ref]
Mast cells, asthma, and PAI-1:
Mast cells induce PAI-1 expression in endothelial cells.[ref] In asthma, mast cell activation causes the release of histamine and proteases that contribute to asthma symptoms.[ref] Mast cells also play a role in tissue fibrosis in asthma, and PAI-1 is thought to be part of this pathway.[ref] More PAI-1 leads to fibrosis.
Researchers have found that genetic variants that increase PAI-1 levels are associated with more airflow obstruction in asthma patients, along with lower forced expiratory volume (FEV1).[ref]
Related articles: Asthma genes | Mast Cell Activation genes
Endothelial nitric oxide synthase:
PAI-1 has recently been found to bind to endothelial nitric oxide and inhibit its production and bioavailability.[ref] Endothelial nitric oxide is a potent vasodilator, which in turn means that it lowers blood pressure.
While the research here is still quite new, it is important to keep in mind that PAI-1 has functions other than inhibiting tPA and uPA.
Related article: Nitric oxide synthase (NOS3 gene)
COVID-19 and PAI-1:
For the original strain of SARS-CoV-2, patients with severe symptoms had higher PAI-1 levels than those with milder disease. Elevated initial levels were also found to be predictive of disease severity.[ref] Another study also found that PAI-1 and its cofactor vitronectin were elevated in Covid patients when compared to other non-Covid respiratory infections and to healthy individuals. Additionally, the study found that there was increased clot fiber length and branching with decreased clot degradation due to the high PAI-1 activity.[ref]
The S1 spike protein alone “stimulated robust production of PAI-1 by human pulmonary microvascular endothelial cells (HPMECs).”[ref] A cell study in lung epithelial cells showed that the spike protein in combination with TLR2 (toll-like receptor 2, an immune system molecule) “enhances PAI-1 expression, potentially affecting the local coagulation cascade.”[ref]
Stress and cortisol increase PAI-1 expression. Researchers found that blocking the cortisol receptor (MR) prevents the increase in PAI-1 in response to the spike protein.[ref]
Insulin resistance:
One reason for cardiovascular complications in type 2 diabetes may be elevated PAI-1 levels. Insulin resistance causes an increase in PAI-1 production.[ref][ref]
PAI-1 levels are also elevated in some people with obesity.[ref] PAI-1 is made in the liver, and fatty liver may be the reason why PAI-1 is elevated in insulin resistance and obesity.[ref][ref]
Related articles: Insulin resistance genes | Fatty liver genes
PAI-1 and pregnancy complications:
During pregnancy, PAI-1 levels naturally increase, which increases coagulation and clotting factors. PAI-1 levels increase gradually in a healthy pregnancy, reaching a maximum level at 32-40 weeks. Levels return to normal a month or two after delivery.
Women with higher-than-normal PAI-1 levels have an increased relative risk of miscarriage, pre-eclampsia, and gestational diabetes.[ref]
Genetics and PAI-1:
The SERPINE1 gene encodes plasminogen activator inhibitor-1 (PAI-1). A number of genetic variants have been identified in the SERPINE1 gene that affect an individual’s natural propensity toward higher or lower PAI-1 levels.
PAI-1 4G/5G Polymorphism:
A common variant in PAI-1 is called 4G/5G due to a repeated section in the promoter region of the SERPINE1 gene, which codes for PAI-1. The PAI-1 5G allele is the more common allele; however, the 4G variant is fairly common, found in around 35% of the population, depending on the ancestry group. The repeated section is linked to two different rs ids, rs1799768 (below in the genotype report) and rs1799889.
Some fertility websites link the PAI-1 4G allele to an increased relative risk of recurrent miscarriages. However, not all studies agree. An analysis of studies on PAI-1 4G/5G for placenta-mediated pregnancy complications showed that in 32 out of 59 studies, there was no increased risk of complications.[ref] It’s possible that the association between PAI-1 4G and miscarriage interacts with other genetic variants that are common in certain ancestry groups, or it could be an interaction with an environmental or dietary factor.
Before taking any medical action, talk to your fertility doctor about how the variant may affect your specific situation.
Can you determine the PAI-1 4G / 5G polymorphism from your 23andMe or Ancestry raw data?
A PAI-1 4G marker SNP is available in 23andMe version 4 data, which you can see below in the genotype report if you have that version of raw data. To know which version of 23andMe raw data you have, look at the filename of your downloaded file. At the end of the filename, it will say v4_full.txt for the version 4 data. If it says “v5”, you have the newer version 5 data file that doesn’t appear to have the PAI-1 4G information.
In addition, there are other genetic polymorphisms that also affect PAI-1 levels, and these variants are included in 23andMe v5 and AncestryDNA raw data. These variants are found primarily in the promoter region of the gene and generally shift the balance toward less fibrinolysis, which increases clotting risk. (See the genotype report section below for your genes.)
There are also a few rare mutations known in PAI-1 that cause deficiency, which then increases the risk of bleeding disorders.
PAI-1 Genotype report:
The SERPINE1 gene encodes plasminogen activator inhibitor-1 (PAI-1).
Access this content:
An active subscription is required to access this content.
Lifehacks:
If you are trying to reduce fibrosis or clotting, inhibiting PAI-1 may be helpful. However, keep in mind that this could also cause increased bleeding risk. Please talk with your doctor or pharmacist about drug interactions if you are taking any medications before starting a supplement.
Dietary and Lifestyle Interventions:
Omega-6 fats may cause higher PAI-1:
A cell study showed that saturated fats (palmitic acid and stearic acid) had no effect on PAI-1 expression. However, omega-6 polyunsaturated fats and omega-3 EPA caused a significant increase in PAI-1.[ref] Another study showed that both stearic acid (saturated fat) and oleic acid (omega-9 in olive oil) had no effect on PAI-1 levels. Other studies back this up, showing that saturated fat does not cause an increase in PAI-1, and that monounsaturated and polyunsaturated fats both increase PAI-1 at least a little bit.[ref][ref] Not all studies agree here. One study of both Japanese and American men found that those with higher serum levels of linoleic and arachidonic acid (omega-6 oils) had lower PAI-1 levels.[ref]
My takeaway: Doctors often recommend cutting out saturated fat for cardiovascular disease, but cutting down on saturated fat may not be effective for people with genetically higher PAI-1, if that is the cause of their heart problems.
Cut the sugar and soda:
One dietary interaction that seems more straightforward is that PAI-1 levels decrease on a low-glycemic-index diet (compared to a high-glycemic-index diet).[ref] Another study suggests that high fructose intake causes higher PAI-1 levels, along with fatty liver disease.[ref]
Regular exercise:
In people with PAI-1 4G/4G, regular exercise helped to reduce PAI-1 levels by 36%.[ref] Another clinical trial in people with fatty liver disease showed that exercise reduced PAI-1 levels significantly.[ref]
Natural PAI-1 inhibitors:
A number of natural compounds have been shown in studies to modulate PAI-1 levels – decreasing high levels without taking it to the extreme of bleeding risk. Always talk with your doctor, though, if you are on any medications (especially blood thinners) before adding in a supplement.
Access this content:
An active subscription is required to access this content.
Related articles:
Nattokinase and Lumbrokinase: Natural Supplements for Clotting and Heart Health
References:
Abdelhakim, Mohamed, and Toshio Miyata. “Plasminogen Activator Inhibitor-1 as a Therapeutic Target for Healthy Longevity, Immunosenescence, and Age-Related Disease: Translational Development of the Small-Molecule Inhibitor TM5614.” Cells, vol. 15, no. 10, May 2026, p. 941. DOI.org (Crossref), https://doi.org/10.3390/cells15100941.
Bahi, Amine, and Jean-Luc Dreyer. “TM5441, a PAI-1 Inhibitor, Attenuates Chronic Stress-Induced Anxio-Depressive-like Behaviors by Restoring the Hippocampal PAI-1/tPA/BDNF Axis.” Psychopharmacology, May 2026. Springer Link, https://doi.org/10.1007/s00213-026-07091-y.
Martínez-Gómez, Laura Edith, et al. “The Fatal Contribution of Serine Protease-Related Genetic Variants to COVID-19 Outcomes.” Frontiers in Immunology, vol. 15, Mar. 2024, p. 1335963. PubMed Central, https://doi.org/10.3389/fimmu.2024.1335963.
Ferraresso, Francesca, Chad W. Skaer, Zimu Wei, Woosuk S. Hur, Hongyin Y, et al. “Age-Associated Increases in PAI-1 Silenced with siRNA-Lipid Nanoparticles Reduces Thrombosis and Prolongs Lifespan.” Blood, vol. 147, no. 18, Apr. 2026, pp. 2053–63. PubMed Central, https://doi.org/10.1182/blood.2025029834.
Oishi, Kyohei, et al. “PAI-1 Inhibitor TM5441 Attenuates Emphysema and Airway Inflammation in a Murine Model of Chronic Obstructive Pulmonary Disease.” International Journal of Molecular Sciences, vol. 26, no. 15, July 2025, p. 7086. DOI.org (Crossref), https://doi.org/10.3390/ijms26157086.