Key Takeaways:
- Inclusion body myositis is a progressive, chronic condition that causes muscle weakness from inflammation in the muscles.
- Inclusion body myositis can be caused by misfolded proteins, autoimmune diseases, and genetic variants.
- Genetic variants related to the immune system are identified as increasing the relative risk of IBM.
Members will see their genotype report below and the solutions in the Lifehacks section. Consider joining today.What is inclusion body myositis (IBM)?
Inclusion body myositis is a progressive, chronic condition that causes muscle weakness. The muscle weakness slowly progresses and causes difficulty climbing stairs, walking, lifting things, and swallowing.
Men are three times more likely to have inclusion body myositis than women, and symptoms often begin in the 50s or early 60s. While a rare condition, it is more commonly found in people in Norway, Western Australia, Minnesota (US), and Japan.[ref]
Sporadic inclusion body myositis:
Inclusion body myositis (IBM) is an inflammatory myopathy, which means it is a disorder that causes inflammation in the muscles. (“Myo” = muscles; “itis” = inflammation)[ref]
The term ‘sporadic’ here means it arises randomly or due to a currently unknown cause. It differentiates the later in life form of inclusion body myositis from the inherited form that tends to occur earlier in life. (More on the inherited form below.)
The main initial symptoms of inclusion body myositis are weakness in the fingers and wrists, and weakness in the quadriceps and ankles. Initial diagnosis can be difficult and often misdiagnosed as arthritis or polymyositis.[ref] Additionally, muscles involved in swallowing and facial movement can be impacted.[ref]
Pathological Features in IBM Pathology Marker Role in IBM Inflammation Immune cells infiltrate muscle fibers Misfolded Proteins Amyloid-beta, tau, alpha-synuclein buildup Mitochondrial Abnormalities mtDNA deletion, mitochondrial dysfunction Increased Autophagy Failure to clear cellular waste NLRP3 Inflammasome Drives excessive inflammation Let’s take a look at each of these characteristics seen in IBM in more depth.
Muscle tissue changes: Inflammation and rimmed vacuoles
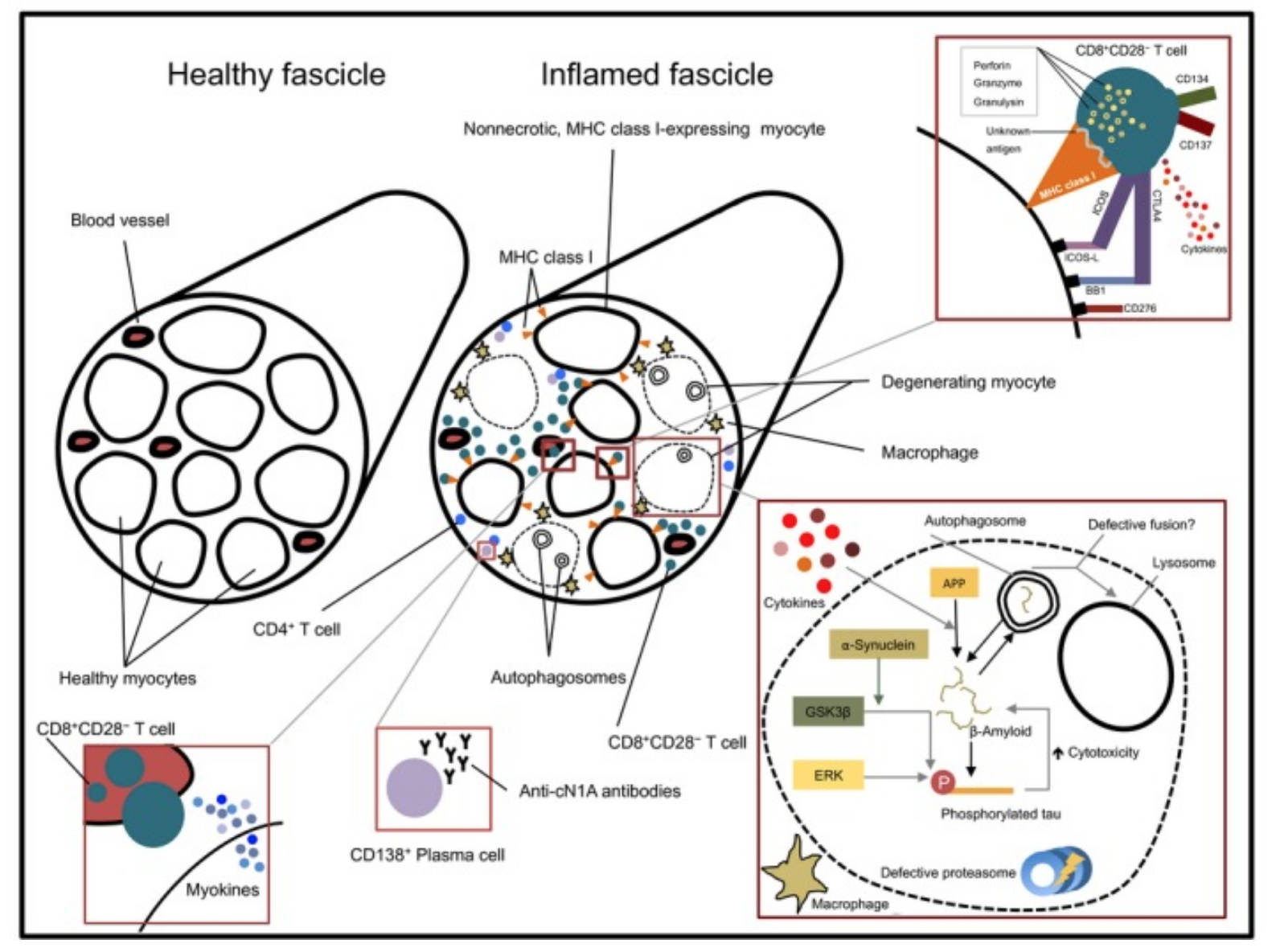
Biopsies of the muscles impacted by IBM showed inflammation surrounding the muscle fibers. Macrophages and T cells invade the muscle fibers. Additionally, there can be mitochondrial changes in the muscle fibers as well as atrophic fibers.[ref]
Another hallmark of IBM is the formation of rimmed vacuoles and the accumulation of misfolded proteins. It points to an increase in autophagy pathways.[ref]
This image from an overview of IBM shows the changes in the muscle tissue (CC license):
Misfolded proteins:
Similar to age-related neurodegenerative diseases, the muscle tissue in people with IBM shows an accumulation of amyloid-beta protein, tau tangles, and alpha-synuclein. These proteins are ‘myotoxic‘ in the muscle tissue. When accumulated in the brain, these proteins cause Alzheimer’s and Parkinson’s diseases.[ref]
Increased NLRP3 inflammasome activation:
When NRLP3 is activated, an inflammasome assembles and increases the inflammatory response in the cell and tissue. It’s like a knob that turns up the volume on inflammation.
In IBM muscle biopsies, researchers found increased NLRP3 expression and immunoreactivity in both inflammatory cells and muscle fiber tissue. The researchers found that damaged mitochondria and altered mitophagy (autophagy for mitochondria) trigger the increase in NLRP3 and inflammasome activation.[ref]
Related article: NLRP3 Gene Variants
Increased autophagy:
Autophagy is how the body breaks down and recycles different components in the cell. It is often likened to taking out the trash and recycling. The overexpression of proteins associated with autophagy is found in muscle biopsies of sporadic inclusion body myositis.[ref]
In addition to recycling and removing misfolded proteins, defective mitochondria are also broken down via autophagy (called mitophagy). Research is still ongoing on how and why autophagy is disordered in IBM.
Related article: Autophagy genes
Mitochondrial DNA deletion:
Mitochondria produce the ATP (energy) needed to power your cells, and muscle cells need a lot of energy. Within the mitochondria, there is mitochondrial DNA that codes for the specific mitochondrial proteins that make up the electron transport chain.
Muscle biopsies for IBM show mitochondrial DNA deletions that affect cytochrome C oxidase, an integral part of the electron transport chain and ATP production. These mtDNA deletions can then be copied throughout clumps of myofibers. Other studies show a decrease in total mtDNA in the muscle.[ref]
Is IBM an autoimmune or degenerative disease?
It is not yet clear to researchers whether IBM (inclusion body myositis) is an autoimmune disease – or – if it is a degenerative disease with inflammation.[ref]
Some researchers believe it is an autoimmune disease because people with IBM often have T cell abnormalities. Genetic research shows that the sporadic form of IBM is associated with known risk factors for autoimmune diseases.[ref]
Bringing this all together:
Like many complex diseases, there is likely not a simple answer to the cause of IBM. Instead, it may be an interplay between inflammation, the dysregulation of proteins, mitochondrial dysfunction, and changes to autophagy. Somewhere in the mix, autoimmunity may be triggering it.
Inclusion body myopathy: Rare hereditary forms of muscle weakness
Inclusion body myopathy 2 is a genetic disease caused by mutations in the GNE gene. The GNE gene codes for an enzyme essential for creating sialic acid. People with two copies of mutations in the GNE gene can have lower levels of a type of sialic acid needed to produce certain cell-signaling proteins in muscle cells.[ref][ref]
Inclusion body myopathy isn’t the same as inclusion body myositis, although both cause similar muscle weakness symptoms.
- Inclusion body myopathy familial (genetic) forms can start affecting an individual earlier, such as in early adulthood.
- Inflammation is not a big component of the hereditary form of inclusion body myopathy 2. Instead, the muscle biopsies show small fibers as well as protein misfolding.[ref]
Ruling out the genetic forms of muscle weakness is likely to be a part of your diagnosis of inclusion body myositis. Some of the genetic mutations for inclusion body myopathy 2 are included below.
Inclusion Body Myositis Genotype Report
Access this content:
An active subscription is required to access this content.
Lifehacks:
If you have inclusion body myositis, please talk to your doctor before making any changes to your diet or lifestyle.Lifestyle and Diet Changes:
The following lifestyle and diet changes have research showing that they may be helpful in IBM.
Exercise:
Several small studies on mild to moderate exercise show that it may help prevent some of the loss of muscle strength in people with IBM.[ref]Ketogenic diet:
A case study of a 54-year-old woman with IBM showed that a low-carb, high-fat ketogenic diet helped to maintain strength, improve walking, and increase the quality of life.[ref]Overall healthy diet:
The Myositis Association recommends a ‘healthy diet’ as necessary… Their recommendations include avoiding processed food, reducing sugar and flour intake, and eating vegetables and fish.[ref] (To me, this seems to be an obvious starting point that most people with IBM are likely already doing.)Supplements for inclusion body myositis:
Access this content:
An active subscription is required to access this content.
Getting more information on inclusion body myositis:
Several organizations are working to raise awareness and help fund research on IBM. These websites are great sources of information on upcoming clinical trials, where to get help, and funding of research studies.
- GettingUp.org – Helping to find treatment and bring awareness of IBM and muscle disorders
- CureIBM – https://cureibm.org/
- The Myositis Association – supporting patients and research for all types of myositis, including IBM
Related Article and Topics:
TNF-alpha: Inflammation, Chronic Diseases, and Genetic Susceptibility
References:
Alfano, Lindsay N., and Linda P. Lowes. “Emerging Therapeutic Options for Sporadic Inclusion Body Myositis.” Therapeutics and Clinical Risk Management, vol. 11, Sept. 2015, pp. 1459–67. PubMed Central, https://doi.org/10.2147/TCRM.S65368.Bayraktar, Oznur, et al. “IBMPFD Disease-Causing Mutant VCP/P97 Proteins Are Targets of Autophagic-Lysosomal Degradation.” PLoS ONE, vol. 11, no. 10, Oct. 2016, p. e0164864. PubMed Central, https://doi.org/10.1371/journal.pone.0164864.
Britson, Kyla A., et al. “New Developments in the Genetics of Inclusion Body Myositis.” Current Rheumatology Reports, vol. 20, no. 5, Apr. 2018, p. 26. PubMed Central, https://doi.org/10.1007/s11926-018-0738-0.
“Diet and Nutrition.” The Myositis Association, https://www.myositis.org/about-myositis/treatment-disease-management/complementary-and-self-care-therapies/diet-and-nutrition/. Accessed 27 June 2022.
Fernández-Martínez, J., et al. “Robust Sampling of Altered Pathways for Drug Repositioning Reveals Promising Novel Therapeutics for Inclusion Body Myositis.” Journal of Rare Diseases Research & Treatment, 2019. Semantic Scholar, https://doi.org/10.29245/2572-9411/2019/2.1174.
Girolamo, F., et al. “Overexpression of Autophagic Proteins in the Skeletal Muscle of Sporadic Inclusion Body Myositis.” Neuropathology and Applied Neurobiology, vol. 39, no. 7, Dec. 2013, pp. 736–49. PubMed, https://doi.org/10.1111/nan.12040.
—. “Overexpression of Autophagic Proteins in the Skeletal Muscle of Sporadic Inclusion Body Myositis.” Neuropathology and Applied Neurobiology, vol. 39, no. 7, Dec. 2013, pp. 736–49. PubMed, https://doi.org/10.1111/nan.12040.
Greenberg, Steven A. “Inclusion Body Myositis: Clinical Features and Pathogenesis.” Nature Reviews Rheumatology, vol. 15, no. 5, May 2019, pp. 257–72. www.nature.com, https://doi.org/10.1038/s41584-019-0186-x.
Güttsches, Anne-Katrin, et al. “Proteomics of Rimmed Vacuoles Define New Risk Allele in Inclusion Body Myositis.” Annals of Neurology, vol. 81, no. 2, Feb. 2017, pp. 227–39. PubMed Central, https://doi.org/10.1002/ana.24847.
Huizing, Marjan, and Donna M. Krasnewich. “Hereditary Inclusion Body Myopathy: A Decade of Progress.” Biochimica et Biophysica Acta (BBA) – Molecular Basis of Disease, vol. 1792, no. 9, Sept. 2009, pp. 881–87. ScienceDirect, https://doi.org/10.1016/j.bbadis.2009.07.001.
“Inclusion-Body Myositis (IBM) – Diseases.” Muscular Dystrophy Association, 18 Dec. 2015, https://www.mda.org/disease/inclusion-body-myositis.
Keller, Christian W., et al. “Immune and Myodegenerative Pathomechanisms in Inclusion Body Myositis.” Annals of Clinical and Translational Neurology, vol. 4, no. 6, May 2017, pp. 422–45. PubMed Central, https://doi.org/10.1002/acn3.419.
Mendell, Jerry R., et al. “Follistatin Gene Therapy for Sporadic Inclusion Body Myositis Improves Functional Outcomes.” Molecular Therapy, vol. 25, no. 4, Apr. 2017, pp. 870–79. ScienceDirect, https://doi.org/10.1016/j.ymthe.2017.02.015.
Muth, Ingrid E., et al. “HMGB1 and RAGE in Skeletal Muscle Inflammation: Implications for Protein Accumulation in Inclusion Body Myositis.” Experimental Neurology, vol. 271, Sept. 2015, pp. 189–97. ScienceDirect, https://doi.org/10.1016/j.expneurol.2015.05.023.
Naddaf, Elie, et al. “Inclusion Body Myositis: Update on Pathogenesis and Treatment.” Neurotherapeutics, vol. 15, no. 4, Oct. 2018, pp. 995–1005. Springer Link, https://doi.org/10.1007/s13311-018-0658-8.
Needham, Merrilee, and Frank L. Mastaglia. “Inclusion Body Myositis.” International Neurology, edited by Robert P. Lisak et al., John Wiley & Sons, Ltd, 2016, pp. 505–07. DOI.org (Crossref), https://doi.org/10.1002/9781118777329.ch122.
Nemunaitis, Gregory, et al. “Hereditary Inclusion Body Myopathy: Single Patient Response to Intravenous Dosing of GNE Gene Lipoplex.” Human Gene Therapy, vol. 22, no. 11, Nov. 2011, pp. 1331–41. liebertpub.com (Atypon), https://doi.org/10.1089/hum.2010.192.
NM_001128227.2(GNE):C.1985C>T (p.Ala662Val) AND Sialuria – ClinVar – NCBI. https://www.ncbi.nlm.nih.gov/clinvar/RCV000265100.1/. Accessed 27 June 2022.
Phillips, Matthew C. L., et al. “Impact of a Ketogenic Diet on Sporadic Inclusion Body Myositis: A Case Study.” Frontiers in Neurology, vol. 11, 2020. Frontiers, https://www.frontiersin.org/article/10.3389/fneur.2020.582402.
Rojana-udomsart, Arada, et al. “Analysis of HLA-DRB3 Alleles and Supertypical Genotypes in the MHC Class II Region in Sporadic Inclusion Body Myositis.” Journal of Neuroimmunology, vol. 254, no. 1–2, Jan. 2013, pp. 174–77. PubMed, https://doi.org/10.1016/j.jneuroim.2012.09.003.
VCV000008474.21 – ClinVar – NCBI. https://www.ncbi.nlm.nih.gov/clinvar/variation/8474/. Accessed 27 June 2022.