Key takeaways:
- Heart disease is the leading cause of death in the US and around the world, and high LDL-cholesterol levels have been linked in many studies to increased heart disease.
- Cholesterol is essential and needed in your cells, in the right amounts.
- Common genetic variants (PCSK9, APOB, LDLR) can cause high cholesterol, especially in combination with dietary choices.
- Specific natural supplements or diet changes may work better for you, depending on your genetic variants. Learn which options may be best with your genes.
Who is this for? If your LDL is high and you’ve run 23andMe/Ancestry, this guide helps you connect specific variants to targeted diet and supplement options. This is educational only, not individual medical advice; work with your physician for treatment decisions.
Members will see their genotype report below, plus additional solutions in the Lifehacks section. Join today.
What LDL cholesterol does in your body
When you read about cholesterol and heart disease, it is easy to believe that cholesterol is something terrible that you don’t want in your body. But that is far from the whole picture! Cholesterol is essential for your health and well-being.
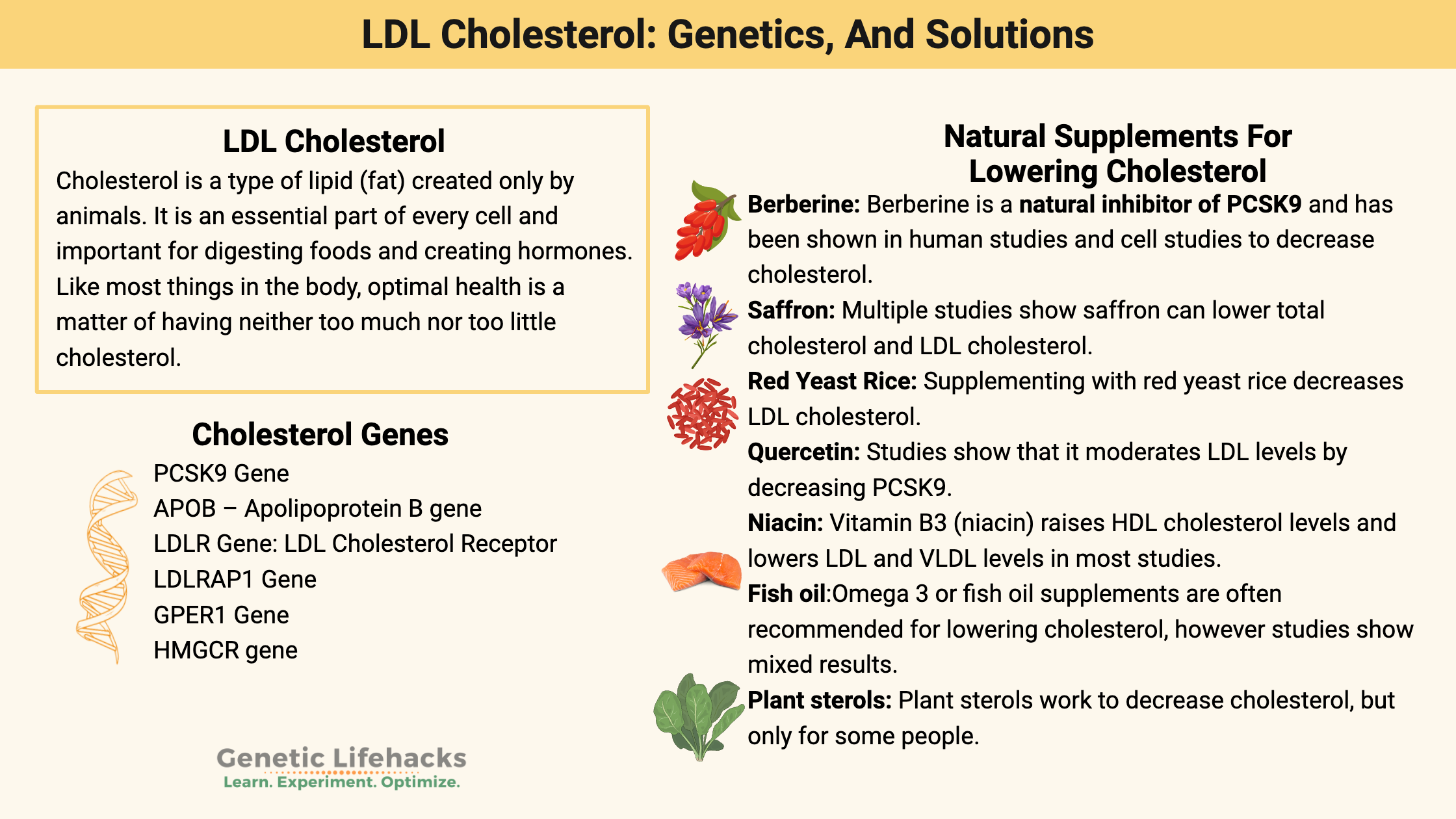
Cholesterol is a type of lipid (fat) created only by animals. It is an essential part of every cell, important for digesting food, creating hormones, and synthesizing vitamin D.
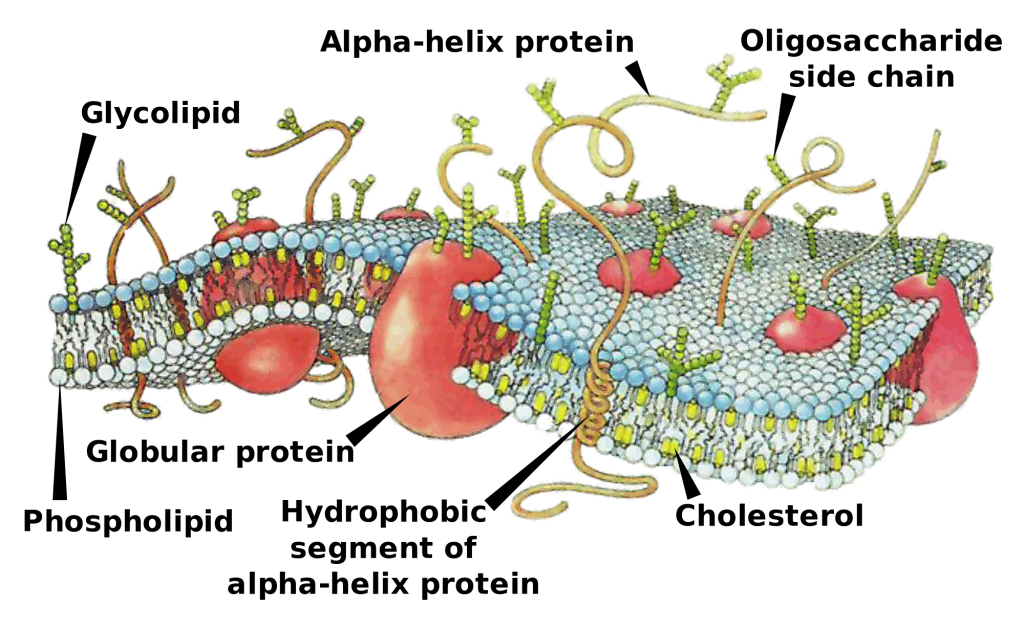
A membrane composed mainly of phospholipids surrounds every cell in your body. Cholesterol molecules make up part of that cell membrane, stabilizing the membrane to help maintain its integrity. Cholesterol keeps the membrane firm enough to keep some very small water-soluble molecules out, yet not too rigid.
In addition to being part of the structure of cells, cholesterol is also the precursor for bile acids, vitamin D, and steroid hormones.
- Bile acids are essential for digesting fats in the diet
- Vitamin D plays a significant role in calcium metabolism and bone health.
- The steroid hormones include testosterone, estrogen, progesterone, cortisol, and aldosterone.
What is a healthy LDL cholesterol level?
Like most things in the body, optimal health is a matter of having neither too much nor too little cholesterol. The right amount is personal, and it depends on our genes, diet, age, and lifestyle.
Below is a chart showing that mortality is lowest in people with an LDL level of a little over 100. The chart shows a sharp increase in mortality with low cholesterol levels and with really high cholesterol levels – a J shaped curve. One reason for the high mortality rates with low cholesterol is that cholesterol helps protect against infectious diseases.[ref] Somewhat higher cholesterol is also associated with a lower risk of diabetes.
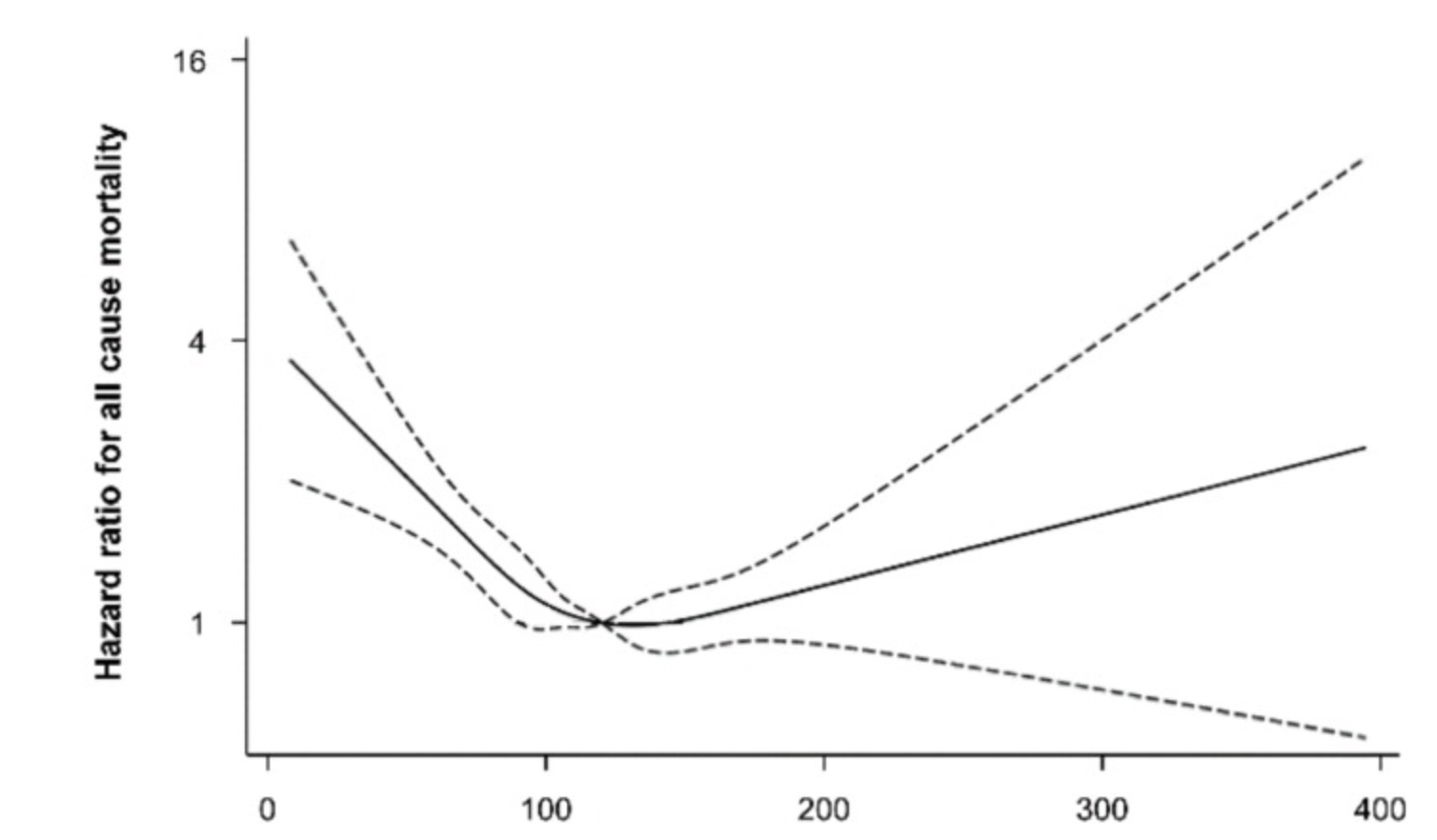
A large 10-year study out of Norway found the lowest mortality rates occurred in people with cholesterol levels between ~190 to 270 mg/dl (5 and 7 mmol/l).[ref]
The CDC and many other health organizations, though, have a narrower range of what they consider healthy.
The CDC range for healthy cholesterol is:[ref]
- Total cholesterol: Under 200 mg/dL is normal
- LDL cholesterol: Under 100 mg/dL is normal
- HDL cholesterol: Best to have more than 40 mg/dL
- Triglycerides: Normal is below 150 mg/dL
These ranges vary in other countries, and the ‘normal’ level changes periodically. For example, according to a JAMA article, normal cholesterol ranged from 240 mg/dL in 1986 and up to 260 mg/dL in 1983.[ref]
Where does cholesterol come from (diet vs synthesis)?
There are two sources of cholesterol:
- Cholesterol in foods
- Cholesterol that your body makes
In addition to the cholesterol that your body makes, cholesterol from food (animal products) is absorbed in the intestines. Eating foods that contain cholesterol causes a temporary increase in serum cholesterol levels, with levels dropping to baseline in about seven hours.[ref]
Generally, eating cholesterol causes the body to produce less of it, and decreasing your cholesterol intake will trigger the body to make more of it. This doesn’t hold true for everyone, but this is the way that it usually works.
Most cholesterol in the body is synthesized in the liver, intestines, adrenals, and reproductive organs. It is a multi-step, complex process to make it.
The regulation of cholesterol synthesis occurs through several processes, with one of the main regulators being the SREBP protein, coded for by the SREBF1 and SREBF2 genes. Other genes involved in your cholesterol levels include cholesterol transport and receptor genes.
How is cholesterol stored?
Cholesterol can be stored in fat droplets packaged with triglycerides and lipoproteins. Chylomicrons are created from dietary fats and contain apolipoproteins, triglycerides, and cholesterol. The backbone of chylomicrons is ApoB. Chylomicrons are taken up by the lymphatic system and then transferred to the blood circulation. Once in circulation, chylomicrons incorporate into adipose (fat) or muscle tissue.[ref]
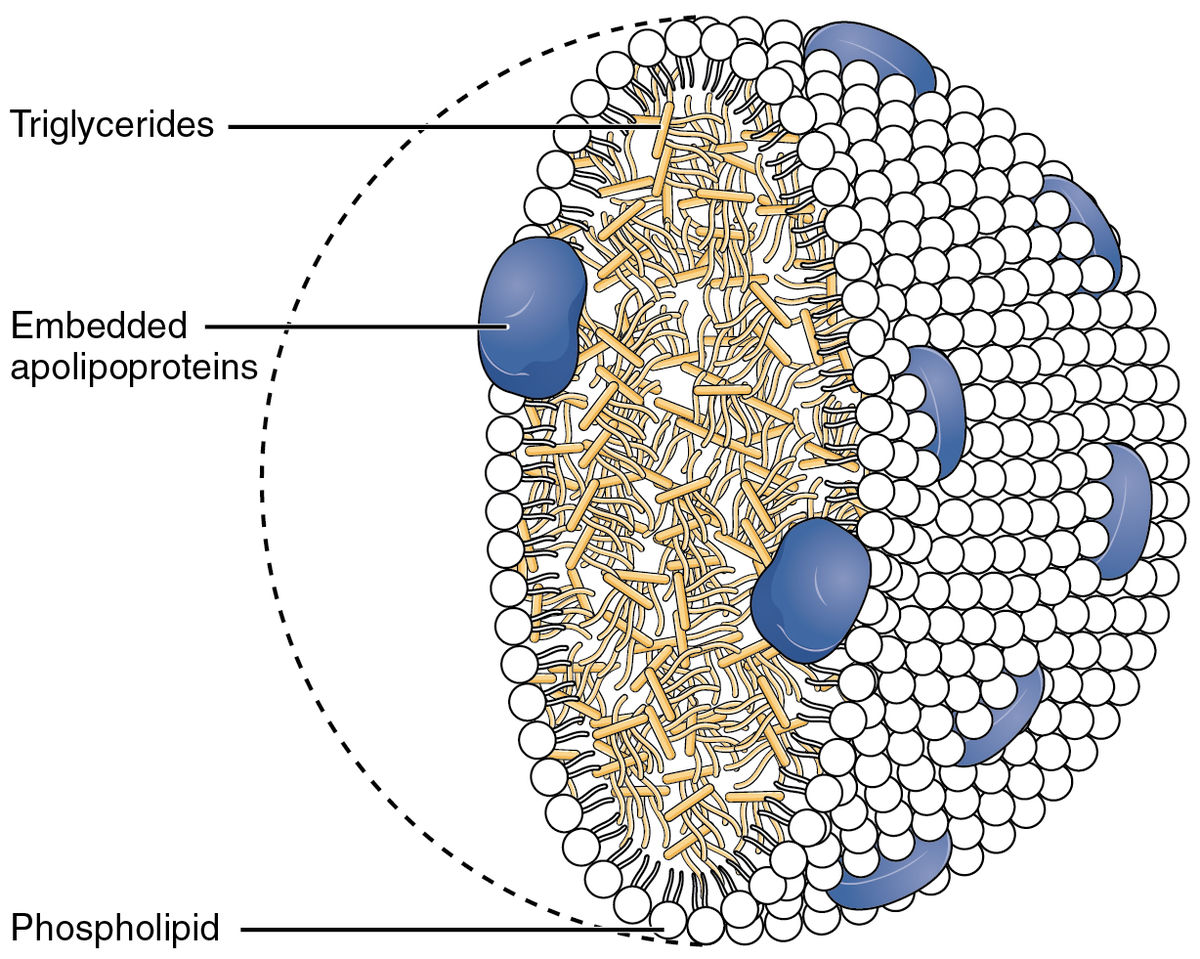
Additionally, cholesterol can be made in the liver and packaged into LDL particles of different densities and sizes, such as VLDL (very low-density lipoprotein) particles. These circulating LDL particles can then bind to cells with an LDL receptor to be utilized by the cell.
How is cholesterol used?
Cholesterol levels are tightly regulated by cells.
LDL receptors control the uptake, and the cell then controls how many LDL-Rs are available via a couple of proteins, including PCSK9.
When excess cholesterol is available, excretion through the liver into the feces occurs. This process is called reverse cholesterol transport. The ABCA1 protein is responsible for moving cholesterol back out of the cells.
See the genotype report section for more on how these genes impact your cholesterol levels.
Does high LDL cholesterol cause heart disease?
According to the CDC, LDL, or ‘bad’ cholesterol, increases heart disease and stroke risk. They recommend eating “foods with plenty of fiber, such as oatmeal and beans, and healthy unsaturated fats, such as avocados, olive oil, and nuts.”[ref]
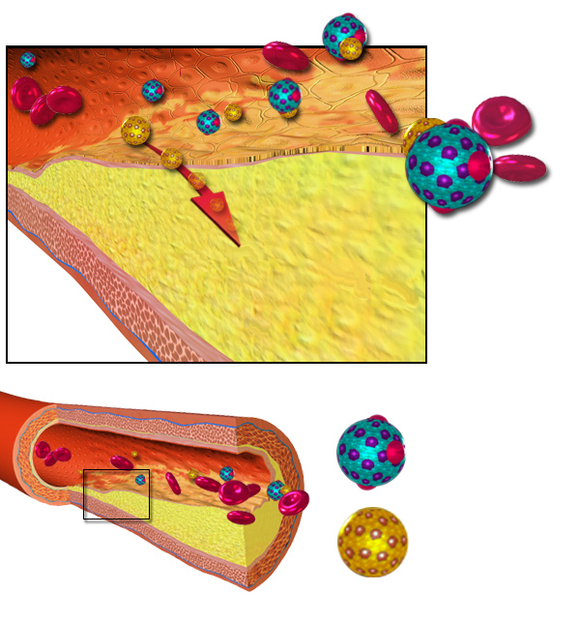
One reason that LDL is linked to heart attacks is that cholesterol is a component of plaques that can build up in the arteries. When the cells lining the blood vessels (endothelial cells) become inflamed, LDL particles are included in the layers of the arteries. When the LDL cholesterol becomes oxidized by reactive oxygen species, it increases inflammation in the vessel.[ref]
It’s too simplistic to say that LDL-c is “bad cholesterol” since it is necessary and essential at the right levels. Let’s dig into the research here because the truth isn’t always as black and white as health websites claim.
A 2010 meta-analysis of twenty-six large clinical trials using statins to reduce cholesterol found the following.[ref]
For every 39 mg/dL reduction in LDL cholesterol level:
- All-cause mortality is 10% lower
- Reduced heart attack deaths
- no effect on strokes or cancer
Studies using genetic risk scores (looking at multiple genetic variants related to cholesterol) find that a lifetime of lower cholesterol levels is associated with lower overall mortality risk.[ref]
“Results of the current study indicate that a genetic predisposition to high LDL-C levels contributes to mortality throughout life, including in the oldest old, and a beneficial LDL genetic risk profile is associated with familial longevity.”
On the other hand, some researchers argue that there is no causality between high cholesterol and heart disease.[ref] Naturally, many of the research studies on statins, cholesterol levels, and heart disease are funded by pharmaceutical companies. And the endpoints and definitions of ‘high’ cholesterol make it hard to compare between studies. It makes it easy to create doubt about the link between really high cholesterol and heart disease.
Familial Hypercholesterolemia (FH) Genes:
Genetic mutations can cause what is known as familial hypercholesterolemia or FH, which is lifelong high cholesterol. Estimates show that 1 in 200 people have FH mutations, which increases the risk of heart disease by 20-fold. In adults, LDL-C levels are often over 190 mg/dL in people with FH mutations.[ref][ref]
While this is still an area of active research, so far, mutations have been identified in the PCSK9, APOB, LDLR, and LDLRAP1 genes.
In addition to familial hypercholesterolemia, lipoprotein(a) is another genetic risk factor for heart disease and can be additive with genetically high cholesterol.
Related article: Lp(a) genes
How statins lower LDL and common side effects
Statins, one type of cholesterol-lowering medicine, are among the most prescribed medications in the US and UK. As of 2024, about 35-40% of Americans over age 40 were taking a statin.
Statins work primarily by blocking HMG-CoA reductase, a liver enzyme involved in cholesterol production, reducing how much the liver makes. Inhibiting HMG-CoA lowers LDL cholesterol and also prompts the liver to pull more LDL from the blood. A Cochrane study on atorvastatin found that LDL cholesterol decreased by 37 – 51%.[ref]
However, this doesn’t answer the question of whether statins are beneficial to health or prevent death.
The Number Needed to Treat website has an extensive review of studies on statins, including the significantly increased risk of diabetes and muscle pain. It is a well-crafted assessment of the risks and benefits that concludes that statins’ risks outweigh the benefits for most people. Everyone is unique. For some people, statins increase brain fog and cause reversible memory problems. Talk with your doctor about your specific risks and benefits.
Related article: Statins, genetics, and muscle pain & Statins, brain fog
Statins, GLP-1 reduction, weight, and diabetes.
GLP-1 is the signal released by the intestines to let the brain and pancreas know that you have consumed food. It tells your brain that you’re full (decreases appetite) and signals to the pancreas to release insulin to lower blood sugar.
- Statins have been shown to interact with the gut microbiome to reduce GLP-1. This likely plays a role in insulin resistance.[ref]
- A 2025 study showed that HMGCR is a regulator of GLP-1 secretion.[ref]
Related article: GLP-1 genes
Many studies show that statin use increases the risk of type 2 diabetes by around 2-fold. Simvastatin and atorvastatin were associated with the greatest increase in type 2 diabetes cases.[ref][ref] A large study concluded that atorvastatin, rosuvastatin, pitavastatin, and simvastatin also increased fasting glucose.[ref]
Related article: Type 2 diabetes genes
Recent research on high and low LDL levels
Studies on both high and low LDL cholesterol show a variety of different effects. The studies below are large, high-quality studies that are not industry-funded to bring you a balanced approach to what can be a nuanced topic.
Low cholesterol reduces dementia but increases mortality from sepsis and lung cancer:
- A study of over 100,000 people in Denmark found that having a lifeline lower LDL cholesterol level (1 mmol/L lower) reduced the risk of Alzheimer’s and dementia.[ref]
- A March 2018 study found that lung cancer patients with low cholesterol were at a 61% higher risk of death.[ref]
- Low LDL-C is associated with greater rates of sepsis in the elderly.[ref]
- Low LDL-c is associated with worse outcomes in hemorrhagic strokes.[ref]
High cholesterol links:
- Hypercholesterolemia (LDL-c >190 mg/dL) significantly elevates the risk of atherosclerotic cardiovascular disease (ASCVD). [ref]
- A review in the JAMA found that each “additional 300 mg of dietary cholesterol consumed per day was significantly associated with a higher risk of incident” of cardiovascular disease.[ref]
- A large review in the Lancet recently found that reducing LDL cholesterol reduces the risk of “major vascular events”.[ref]
A picture emerges that LDL levels that are neither lower than normal nor higher than normal are best for overall mortality rates.
Genotype Report: LDL Cholesterol and APOB
PCSK9 Gene: The PCSK9 gene codes for an enzyme involved in cholesterol transport, interacting with the LDL receptors. (Learn more here).
Variants here largely tell you whether LDL‑lowering strategies that upregulate the LDL receptor (e.g., berberine, PCSK9 inhibitors) might be especially effective.
Access this content:
An active subscription is required to access this content.
Lifehacks:
First, confirm what your baseline total cholesterol and LDL levels are with a basic test. If the results are concerning, be sure to talk with your doctor about any medical questions or questions about supplement interactions with prescription medications.
Once you know your baseline level is high, you can work to lower it by:
- Upgrade diet and activity (works for most genotypes)
- Layer targeted supplements (based on your genes and labs)
- Also consider medications or specialist care, especially with FH mutations, LDL >190, or other risk factors.
Modifying Cholesterol with Diet
The old advice to give up eggs to lower your cholesterol is inaccurate, according to research studies[ref]. Similarly, choline from eggs or supplements does not raise cholesterol levels.[ref]
So what works to lower cholesterol? A whole-food diet and moderate exercise are usually beneficial for keeping cholesterol levels in check. Yep – standard advice to cut out fast food and hit the gym a few times per week. Cutting out processed food should decrease inflammation and lower cholesterol levels. Cleaning up the diet does work for most people and is an obvious route to try.[ref][ref]
A meta-analysis that combined the data from a bunch of studies found that fruit and vegetable intake of 3+ servings per day decreases triglyceride levels and improves total cholesterol. (Interestingly, the study found no extra benefit from consuming five or more servings of fruits and vegetables per day.)[ref]
How much does diet matter? Type 2 diabetics on a low-fat vegan diet (lots of fruits and vegetables) had a decrease in cholesterol levels of 13.5 mg/dL.[ref]
Ketogenic Diet and LDL:
A recent study of healthy, normal-weight women found that a low-carb, high-fat ketogenic diet for a month increases LDL cholesterol significantly (~70 mg/dL). The diet was high in saturated fats and low in fiber.[ref]
Keep in mind that individual results will likely vary – the range of increase was between 40 and 90 mg/dL for these study participants.
7 Natural supplements with solid research for lowering cholesterol
Access this content:
An active subscription is required to access this content.
Related Articles and Topics:
References:
Adams, Stephen P., et al. “Atorvastatin for Lowering Lipids.” The Cochrane Database of Systematic Reviews, vol. 2015, no. 3, Mar. 2015.
www.ncbi.nlm.nih.gov, https://doi.org/10.1002/14651858.CD008226.pub3.
Adorni, Maria Pia, et al. “Effect of a Novel Nutraceutical Combination on Serum Lipoprotein Functional Profile and Circulating PCSK9.” Therapeutics and Clinical Risk Management, vol. 13, 2017, pp. 1555–62. PubMed, https://doi.org/10.2147/TCRM.S144121.
Barnard, Neal D., et al. “A Low-Fat Vegan Diet and a Conventional Diabetes Diet in the Treatment of Type 2 Diabetes: A Randomized, Controlled, 74-Wk Clinical Trial.” The American Journal of Clinical Nutrition, vol. 89, no. 5, May 2009, pp. 1588S-1596S. PubMed, https://doi.org/10.3945/ajcn.2009.26736H.
Batuca, Joana R., et al. “Extended-Release Niacin Increases Anti-Apolipoprotein A-I Antibodies That Block the Antioxidant Effect of High-Density Lipoprotein-Cholesterol: The EXPLORE Clinical Trial.” British Journal of Clinical Pharmacology, vol. 83, no. 5, May 2017, pp. 1002–10. PubMed, https://doi.org/10.1111/bcp.13198.
Beheshti, Sabina, et al. “Relationship of Familial Hypercholesterolemia and High Low-Density Lipoprotein Cholesterol to Ischemic Stroke: Copenhagen General Population Study.” Circulation, vol. 138, no. 6, Aug. 2018, pp. 578–89. PubMed, https://doi.org/10.1161/CIRCULATIONAHA.118.033470.
Benito-Vicente, Asier, et al. “Familial Hypercholesterolemia: The Most Frequent Cholesterol Metabolism Disorder Caused Disease.” International Journal of Molecular Sciences, vol. 19, no. 11, Nov. 2018. www.ncbi.nlm.nih.gov, https://doi.org/10.3390/ijms19113426.
—. “Familial Hypercholesterolemia: The Most Frequent Cholesterol Metabolism Disorder Caused Disease.” International Journal of Molecular Sciences, vol. 19, no. 11, Nov. 2018. www.ncbi.nlm.nih.gov, https://doi.org/10.3390/ijms19113426.
Benn, Marianne, Børge G Nordestgaard, et al. “Low LDL Cholesterol, PCSK9 and HMGCR Genetic Variation, and Risk of Alzheimer’s Disease and Parkinson’s Disease: Mendelian Randomisation Study.” The BMJ, vol. 357, Apr. 2017, p. j1648. PubMed Central, https://doi.org/10.1136/bmj.j1648.
Benn, Marianne, Børge G. Nordestgaard, et al. “PCSK9R46L, Low-Density Lipoprotein Cholesterol Levels, and Risk of Ischemic Heart Disease: 3 Independent Studies and Meta-Analyses.” Journal of the American College of Cardiology, vol. 55, no. 25, June 2010, pp. 2833–42. ScienceDirect, https://doi.org/10.1016/j.jacc.2010.02.044.
Calandra, Sebastiano, et al. “Mechanisms and Genetic Determinants Regulating Sterol Absorption, Circulating LDL Levels, and Sterol Elimination: Implications for Classification and Disease Risk.” Journal of Lipid Research, vol. 52, no. 11, Nov. 2011, pp. 1885–926. DOI.org (Crossref), https://doi.org/10.1194/jlr.R017855.
—. “Mechanisms and Genetic Determinants Regulating Sterol Absorption, Circulating LDL Levels, and Sterol Elimination: Implications for Classification and Disease Risk.” Journal of Lipid Research, vol. 52, no. 11, Nov. 2011, pp. 1885–926. DOI.org (Crossref), https://doi.org/10.1194/jlr.R017855.
Cao, Shijie, et al. “Berberrubine and Its Analog, Hydroxypropyl-Berberrubine, Regulate LDLR and PCSK9 Expression via the ERK Signal Pathway to Exert Cholesterol-Lowering Effects in Human Hepatoma HepG2 Cells.” Journal of Cellular Biochemistry, Oct. 2018. PubMed, https://doi.org/10.1002/jcb.27102.
CDC. “Cholesterol Myths and Facts | Cdc.Gov.” Centers for Disease Control and Prevention, 26 Jan. 2021, https://www.cdc.gov/cholesterol/myths_facts.htm.
—. “How and When to Have Your Cholesterol Checked | Cdc.Gov.” Centers for Disease Control and Prevention, 15 Apr. 2021, https://www.cdc.gov/cholesterol/checked.htm.
Chen, Suet N., et al. “A Common PCSK9 Haplotype, Encompassing the E670G Coding Single Nucleotide Polymorphism, Is a Novel Genetic Marker for Plasma Low-Density Lipoprotein Cholesterol Levels and Severity of Coronary Atherosclerosis.” Journal of the American College of Cardiology, vol. 45, no. 10, May 2005, pp. 1611–19. PubMed, https://doi.org/10.1016/j.jacc.2005.01.051.
Chen, Yeda, et al. “Association Between Apolipoprotein B XbaI Polymorphism and Coronary Heart Disease in Han Chinese Population: A Meta-Analysis.” Genetic Testing and Molecular Biomarkers, vol. 20, no. 6, June 2016, pp. 304–11. PubMed, https://doi.org/10.1089/gtmb.2015.0126.
Chikowore, Tinashe, et al. “C679X Loss-of-Function PCSK9 Variant Lowers Fasting Glucose Levels in a Black South African Population: A Longitudinal Study.” Diabetes Research and Clinical Practice, vol. 144, Oct. 2018, pp. 279–85. PubMed, https://doi.org/10.1016/j.diabres.2018.09.012.
Cohen, Jonathan, et al. “Low LDL Cholesterol in Individuals of African Descent Resulting from Frequent Nonsense Mutations in PCSK9.” Nature Genetics, vol. 37, no. 2, Feb. 2005, pp. 161–65. PubMed, https://doi.org/10.1038/ng1509.
—. “Low LDL Cholesterol in Individuals of African Descent Resulting from Frequent Nonsense Mutations in PCSK9.” Nature Genetics, vol. 37, no. 2, Feb. 2005, pp. 161–65. PubMed, https://doi.org/10.1038/ng1509.
—. “Low LDL Cholesterol in Individuals of African Descent Resulting from Frequent Nonsense Mutations in PCSK9.” Nature Genetics, vol. 37, no. 2, Feb. 2005, pp. 161–65. PubMed, https://doi.org/10.1038/ng1509.
Collaboration, Cholesterol Treatment Trialists’ (CTT). “Efficacy and Safety of More Intensive Lowering of LDL Cholesterol: A Meta-Analysis of Data from 170 000 Participants in 26 Randomised Trials.” Lancet, vol. 376, no. 9753, Nov. 2010, p. 1670. www.ncbi.nlm.nih.gov, https://doi.org/10.1016/S0140-6736(10)61350-5.
Dubois, C., et al. “Effects of Increasing Amounts of Dietary Cholesterol on Postprandial Lipemia and Lipoproteins in Human Subjects.” Journal of Lipid Research, vol. 35, no. 11, Nov. 1994, pp. 1993–2007.
Fahed, Akl C., et al. “Variable Expressivity and Co-Occurrence of LDLR and LDLRAP1 Mutations in Familial Hypercholesterolemia: Failure of the Dominant and Recessive Dichotomy.” Molecular Genetics & Genomic Medicine, vol. 4, no. 3, May 2016, pp. 283–91. PubMed, https://doi.org/10.1002/mgg3.203.
—. “Variable Expressivity and Co-Occurrence of LDLR and LDLRAP1 Mutations in Familial Hypercholesterolemia: Failure of the Dominant and Recessive Dichotomy.” Molecular Genetics & Genomic Medicine, vol. 4, no. 3, May 2016, pp. 283–91. PubMed, https://doi.org/10.1002/mgg3.203.
“Familial Hypercholesterolemia.” NORD (National Organization for Rare Disorders), https://rarediseases.org/rare-diseases/familial-hypercholesterolemia/. Accessed 26 Oct. 2021.
Fouladseresht, Hamed, et al. “Association of ABCA1 Haplotypes with Coronary Artery Disease.” Laboratory Medicine, vol. 51, no. 2, Mar. 2020, pp. 157–68. PubMed, https://doi.org/10.1093/labmed/lmz031.
Group, Graham Walker and The NNT. “Statins for Heart Disease Prevention (Without Prior Heart Disease).” TheNNT, http://www.thennt.com/nnt/statins-for-heart-disease-prevention-without-prior-heart-disease/. Accessed 26 Oct. 2021.
Guirgis, Faheem W., et al. “Cholesterol Levels and Long-Term Rates of Community-Acquired Sepsis.” Critical Care, vol. 20, 2026. www.ncbi.nlm.nih.gov, https://doi.org/10.1186/s13054-016-1579-8.
Haghighatdoost, Fahimeh, and Mitra Hariri. “Effect of Resveratrol on Lipid Profile: An Updated Systematic Review and Meta-Analysis on Randomized Clinical Trials.” Pharmacological Research, vol. 129, Mar. 2018, pp. 141–50. PubMed, https://doi.org/10.1016/j.phrs.2017.12.033.
—. “Effect of Resveratrol on Lipid Profile: An Updated Systematic Review and Meta-Analysis on Randomized Clinical Trials.” Pharmacological Research, vol. 129, Mar. 2018, pp. 141–50. PubMed, https://doi.org/10.1016/j.phrs.2017.12.033.
Hayat, Mahtaab, et al. “Genetic Associations between Serum Low LDL-Cholesterol Levels and Variants in LDLR, APOB, PCSK9 and LDLRAP1 in African Populations.” PLoS ONE, vol. 15, no. 2, 2020. www.ncbi.nlm.nih.gov, https://doi.org/10.1371/journal.pone.0229098.
Hubacek, J. A., et al. “Polygenic Hypercholesterolemia: Examples of GWAS Results and Their Replication in the Czech-Slavonic Population.” Physiological Research, vol. 66, no. Suppl 1, Apr. 2026, pp. S101–11. PubMed, https://doi.org/10.33549/physiolres.933580.
Hussain, Yasin, et al. “G-Protein Estrogen Receptor as a Regulator of Low-Density Lipoprotein Cholesterol Metabolism: Cellular and Population Genetic Studies.” Arteriosclerosis, Thrombosis, and Vascular Biology, vol. 35, no. 1, Jan. 2015, pp. 213–21. PubMed, https://doi.org/10.1161/ATVBAHA.114.304326.
Kent, Shia T., et al. “PCSK9 Loss-of-Function Variants, Low-Density Lipoprotein Cholesterol, and Risk of Coronary Heart Disease and Stroke: Data From 9 Studies of Blacks and Whites.” Circulation. Cardiovascular Genetics, vol. 10, no. 4, Aug. 2017, p. e001632. PubMed, https://doi.org/10.1161/CIRCGENETICS.116.001632.
Khera, Amit V., et al. “Diagnostic Yield and Clinical Utility of Sequencing Familial Hypercholesterolemia Genes in Patients With Severe Hypercholesterolemia.” Journal of the American College of Cardiology, vol. 67, no. 22, June 2016, pp. 2578–89. PubMed, https://doi.org/10.1016/j.jacc.2016.03.520.
Khoury, D. El, et al. “Beta Glucan: Health Benefits in Obesity and Metabolic Syndrome.” Journal of Nutrition and Metabolism, vol. 2012, 2012. www.ncbi.nlm.nih.gov, https://doi.org/10.1155/2012/851362.
Kwon, H. J., et al. “Molecular Basis for LDL Receptor Recognition by PCSK9.” Proceedings of the National Academy of Sciences, vol. 105, no. 6, Feb. 2008, pp. 1820–25. DOI.org (Crossref), https://doi.org/10.1073/pnas.0712064105.
Malekmohammad, Khojasteh, et al. “Antioxidants and Atherosclerosis: Mechanistic Aspects.” Biomolecules, vol. 9, no. 8, Aug. 2019. www.ncbi.nlm.nih.gov, https://doi.org/10.3390/biom9080301.
Lee, Kang-Po, and Li-Chi Hsu. “Impact of LDL-C Levels on Severity and Outcome of Intracranial Haemorrhage: A Single-Centre Retrospective Study.” BMJ Neurology Open, vol. 7, no. 1, June 2025, p. e000850. PubMed Central, https://doi.org/10.1136/bmjno-2024-000850.
Mbikay, Majambu, et al. “Mice Fed a High-Cholesterol Diet Supplemented with Quercetin-3-Glucoside Show Attenuated Hyperlipidemia and Hyperinsulinemia Associated with Differential Regulation of PCSK9 and LDLR in Their Liver and Pancreas.” Molecular Nutrition & Food Research, vol. 62, no. 9, May 2018, p. e1700729. PubMed, https://doi.org/10.1002/mnfr.201700729.
Mhaimeed, Omar, et al. “The Importance of LDL-C Lowering in Atherosclerotic Cardiovascular Disease Prevention: Lower for Longer Is Better.” American Journal of Preventive Cardiology, vol. 18, Mar. 2024, p. 100649. PubMed Central, https://doi.org/10.1016/j.ajpc.2024.100649.
Miskelly, Michael G., et al. “HMGCR and Rosuvastatin Regulates GLP-1 Secretion and Expression – a Translational Study.” The Journal of Clinical Endocrinology and Metabolism, Nov. 2025, p. dgaf608. PubMed, https://doi.org/10.1210/clinem/dgaf608.
Moazzen, Hossein, and Mohammad Alizadeh. “Effects of Pomegranate Juice on Cardiovascular Risk Factors in Patients with Metabolic Syndrome: A Double-Blinded, Randomized Crossover Controlled Trial.” Plant Foods for Human Nutrition (Dordrecht, Netherlands), vol. 72, no. 2, June 2017, pp. 126–33. PubMed, https://doi.org/10.1007/s11130-017-0605-6.
Niu, Caiqin, et al. “Associations of the APOB Rs693 and Rs17240441 Polymorphisms with Plasma APOB and Lipid Levels: A Meta-Analysis.” Lipids in Health and Disease, vol. 16, no. 1, Sept. 2017, p. 166. BioMed Central, https://doi.org/10.1186/s12944-017-0558-7.
NM_000384.2(APOB):C.10580G>A (p.Arg3527Gln) AND Familial Hypercholesterolemia – ClinVar – NCBI. https://www.ncbi.nlm.nih.gov/clinvar/RCV000019479.30/. Accessed 26 Oct. 2021.
Petursson, Halfdan, et al. “Is the Use of Cholesterol in Mortality Risk Algorithms in Clinical Guidelines Valid? Ten Years Prospective Data from the Norwegian HUNT 2 Study.” Journal of Evaluation in Clinical Practice, vol. 18, no. 1, Feb. 2012, pp. 159–68. PubMed, https://doi.org/10.1111/j.1365-2753.2011.01767.x.
Postmus, Iris, Joris Deelen, et al. “LDL Cholesterol Still a Problem in Old Age? A Mendelian Randomization Study.” International Journal of Epidemiology, vol. 44, no. 2, Apr. 2015, pp. 604–12. PubMed, https://doi.org/10.1093/ije/dyv031.
Postmus, Iris, Stella Trompet, et al. “PCSK9 SNP Rs11591147 Is Associated with Low Cholesterol Levels but Not with Cognitive Performance or Noncardiovascular Clinical Events in an Elderly Population.” Journal of Lipid Research, vol. 54, no. 2, Feb. 2013, pp. 561–66. PubMed Central, https://doi.org/10.1194/jlr.M033969.
Qiu, Chengfeng, et al. “What Is the Impact of PCSK9 Rs505151 and Rs11591147 Polymorphisms on Serum Lipids Level and Cardiovascular Risk: A Meta-Analysis.” Lipids in Health and Disease, vol. 16, no. 1, June 2017, p. 111. PubMed, https://doi.org/10.1186/s12944-017-0506-6.
Ravnskov, Uffe, et al. “LDL-C Does Not Cause Cardiovascular Disease: A Comprehensive Review of the Current Literature.” Expert Review of Clinical Pharmacology, vol. 11, no. 10, Oct. 2018, pp. 959–70. PubMed, https://doi.org/10.1080/17512433.2018.1519391.
Schucker, B., et al. “Change in Cholesterol Awareness and Action. Results from National Physician and Public Surveys.” Archives of Internal Medicine, vol. 151, no. 4, Apr. 1991, pp. 666–73.
Slimani, Afef, et al. “Effect of E670G Polymorphism in PCSK9 Gene on the Risk and Severity of Coronary Heart Disease and Ischemic Stroke in a Tunisian Cohort.” Journal of Molecular Neuroscience: MN, vol. 53, no. 2, June 2014, pp. 150–57. PubMed, https://doi.org/10.1007/s12031-014-0238-2.
SREBF1 Sterol Regulatory Element Binding Transcription Factor 1 [Homo Sapiens (Human)] – Gene – NCBI. https://www.ncbi.nlm.nih.gov/gene/6720. Accessed 26 Oct. 2021.
“Statins – Prices and Information.” GoodRx, https://www.goodrx.com/statins. Accessed 26 Oct. 2021.
VCV000002873.2 – ClinVar – NCBI. https://www.ncbi.nlm.nih.gov/clinvar/variation/2873/. Accessed 26 Oct. 2021.
Wang, Nelson, et al. “Intensive LDL Cholesterol-Lowering Treatment beyond Current Recommendations for the Prevention of Major Vascular Events: A Systematic Review and Meta-Analysis of Randomised Trials Including 327 037 Participants.” The Lancet. Diabetes & Endocrinology, vol. 8, no. 1, Jan. 2020, pp. 36–49. PubMed, https://doi.org/10.1016/S2213-8587(19)30388-2.
Wang, Yanan, et al. “Barley β-Glucan Reduces Blood Cholesterol Levels via Interrupting Bile Acid Metabolism.” The British Journal of Nutrition, vol. 118, no. 10, Nov. 2017, pp. 822–29. PubMed, https://doi.org/10.1017/S0007114517002835.
Xu, Lin, et al. “Egg Consumption and the Risk of Cardiovascular Disease and All-Cause Mortality: Guangzhou Biobank Cohort Study and Meta-Analyses.” European Journal of Nutrition, vol. 58, no. 2, Mar. 2019, pp. 785–96. PubMed, https://doi.org/10.1007/s00394-018-1692-3.
Zhang, Gu, et al. “Low Serum Levels of Pre-Surgical Total Cholesterol Are Associated with Unfavorable Overall Survival in Patients with Operable Non-Small Cell Lung Cancer.” Clinical Laboratory, vol. 64, no. 3, Mar. 2018, pp. 321–27. PubMed, https://doi.org/10.7754/Clin.Lab.2017.170823.
Zhong, Victor W., et al. “Associations of Dietary Cholesterol or Egg Consumption With Incident Cardiovascular Disease and Mortality.” JAMA, vol. 321, no. 11, Mar. 2019, pp. 1081–95. PubMed, https://doi.org/10.1001/jama.2019.1572.