Key takeaways:
- GLP-1 is a rapid-acting gut hormone that regulates blood sugar and appetite by signaling insulin release and suppressing glucagon.
- GLP-1 controls specific types of appetite rather than baseline hunger. Acute stress and large meals trigger GLP-1 in the brain to suppress appetite, preventing overeating.
- GLP-1 receptor agonist drugs (e.g., semaglutide, liraglutide, tirzapeptide) work by mimicking natural GLP-1 but last much longer.
- Genetic variants in the GLP1-related genes are linked to obesity and diabetes. Variants influence whether someone is likely to respond well to GLP-1 RAs for weight loss.
- Beyond weight loss, GLP-1 RAs show promise for cardiovascular disease, dementia prevention, mast cells, and immune conditions. Side effects are common and of concern, though.
What Is GLP-1 and How Does It Work?
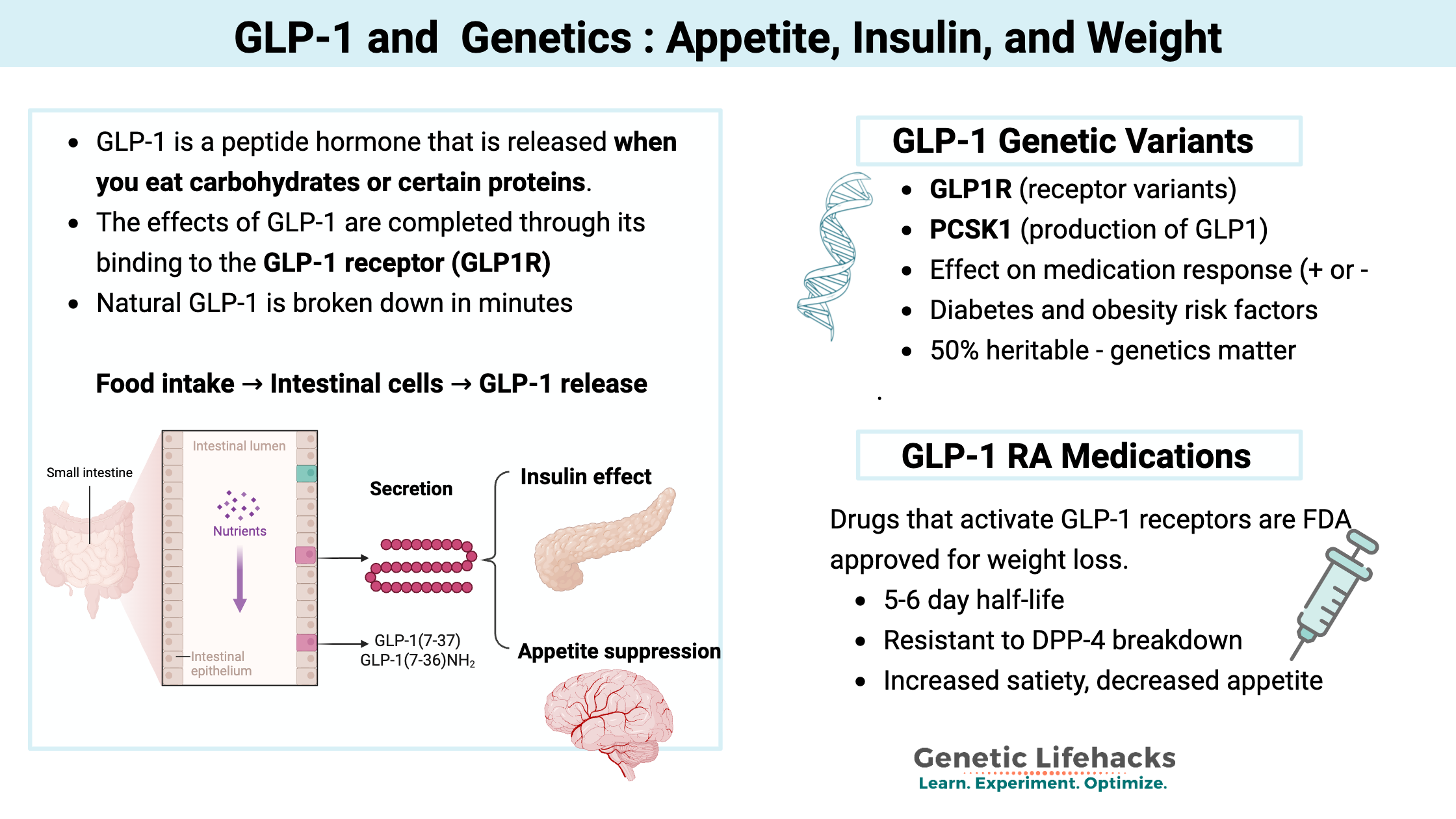
When food reaches your intestine, it triggers the release of hormones that signal to other parts of your body. These signals tell your brain that you’re no longer hungry and prompt the pancreas to release insulin. One of these hormones is GLP-1 (glucagon-like peptide-1).
This article explores how GLP-1 works, how your genes influence GLP-1 levels, and how your genes interact with your response to GLP-1 RA medications for weight loss or diabetes. Current 2026 approved GLP-1 RA medications include semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound).
Gut-brain axis:
GLP-1 is a peptide hormone (a small protein molecule) that is released in the upper part of the intestinal tract when you eat carbohydrates or certain proteins. It is classified as an incretin, which means it is a hormone released to regulate blood glucose levels.
GLP-1 receptors (GLP1R), which are found in pancreatic beta cells as well as other cell types, receive the GLP-1 signal, triggering the release of insulin. GLP-1 receptors are also found in other cells in the pancreas, where the signal then stops the release of glucagon, which prevents the liver from generating glucose.[ref] Additionally, GLP-1 is created in the brain and acts as a neuropeptide.
To understand how GLP-1 works, we first need to look at how the body produces this hormone.
How GLP-1 Is Made (Proglucagon Pathway)
The production of GLP-1 begins with a larger precursor molecule.
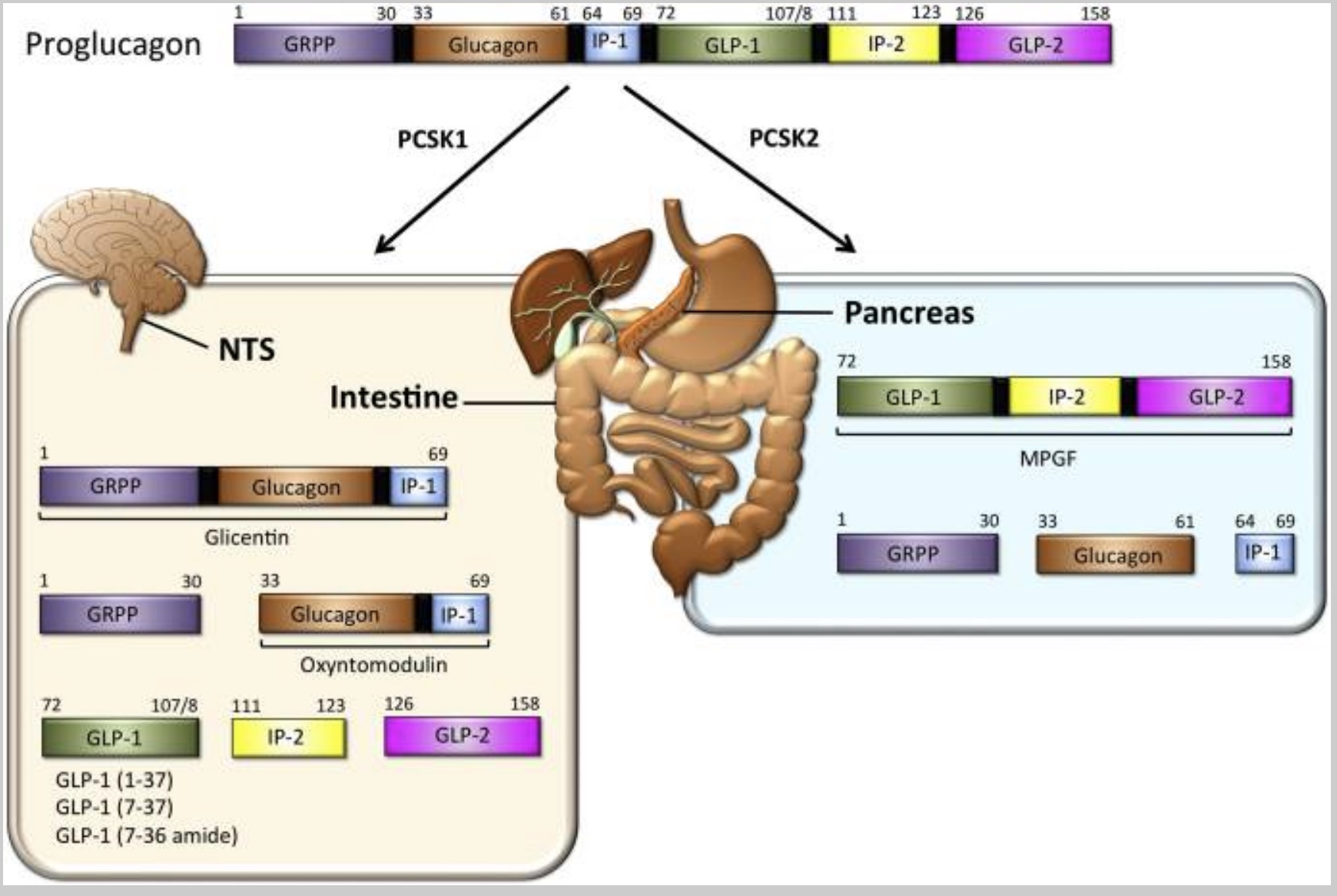
Proglucagon is a large precursor hormone molecule produced in the pancreas (alpha cells) and the intestines. It can be chopped apart to form other molecules — including GLP-1. Preproglucagon is encoded by the GCG gene and cleaved into proglucagon.
Beyond appetite regulation, GLP-1 plays a critical role in blood sugar management.
Controlling glucose levels:
In the pancreas, the proglucagon can convert into glucagon, which in turn signals the liver to release glucose. The alpha cells in the pancreas secrete proglucagon when blood glucose levels are low. The release of proglucagon causes the liver to make glucose (gluconeogenesis – converting protein to glucose) as well as to convert fatty acids into ketone bodies.
Intestinal proglucagon cleaves (breaks up) into several different molecules:
- GLP-1
- GLP-2
- GRPP
- Oxyntomodulin
The enzyme PCSK1 converts proglucagon to GLP-1 in the central nervous system. (We’ll come back to this in the genetics section)
The following diagram illustrates how proglucagon is cleaved into its various components:
Why GLP-1 Is Broken Down So Fast (DPP-4)
The GLP-1 hormone has a remarkably short half-life of around 2 minutes. This quick signal is rapidly degraded by the protein DPP-4 (dipeptidyl peptidase 4).
As a result of this rapid degradation, only about 10-15% of released GLP-1 reaches the pancreas intact. Blocking the degradation of GLP-1 by inhibiting DPP-4 is how certain types of diabetes medicine work.
The GLP-1 that does reach the pancreas calls for the release of more insulin when food is being broken down and absorbed. Plus, it stops the production of glucagon, thus decreasing glucose from the liver.
The effects of GLP-1 are mediated through its binding to the GLP-1 receptor (GLP1R).
GLP-1 and the Gut Microbiome:
The focus with weight loss and diabetes is the spike in GLP-1 after eating that is quickly broken down. This spike is the signal to the pancreas for insulin release and the full signal to the brain.
However, we also have a constant, low level of circulating GLP-1 even when fasting.[ref][ref] This directly ties into the gut microbiome. A healthy gut microbiome with diversity produces short-chain fatty acids, causing GLP-1 release. Bile acids can also stimulate GLP-1.[ref]
Importantly, modern exposure to glyphosate and antibiotics may be reducing our natural, constant GLP-1 levels:
- Animal studies show that GLP-1 levels are reduced due to gut microbiome changes from glyphosate.[ref]
- Studies using germ-free mice show that GLP-1 secretion after a meal is abolished without the gut microbiome.[ref]
How GLP-1 Controls Appetite and Prevents Binge Eating
GLP-1 regulates appetite through several distinct mechanisms that affect the brain and the gut.
GLP-1 in the Brain: Stress, Satiety, and Food Noise
Different regions in the brain control your desire to eat, and GLP-1 comes into play here in specific ways. The hypothalamus can make GLP-1, as well as regions of the brain stem. Plus, GLP-1 is involved in stress response and the HPA axis.[ref]
The brain stem controls a lot of our basic, involuntary functions, such as heart rate and breathing. Specific neurons in the brain stem control swallowing, intestinal movements — and stress-induced loss of appetite.
GLP-1 in the brain stem is activated due to stress and causes a loss of appetite. Researchers determined this using transgenic mice, allowing them to turn off the GLP-1 in the brain to see what happens. The researchers found that turning off GLP-1 in the brain didn’t affect the normal daily intake of food, but instead was important in several specific situations: prolonged fasting, large feedings, and stress-induced appetite loss.[ref]
- Controlling binging, regulating satiety:
Essentially, the neurons activated by GLP-1 help to limit binging after a fast – they keep you from massively overeating after not eating for a while. The GLP-1-activated neurons in the brain also limit appetite for a while after a large meal (e.g., the thought of eating is unappealing for many hours after pigging out on pizza).[ref] - Stress-related appetite suppression:
Additionally, the GLP-1 neurons activate during times of acute stress to suppress appetite. We all have experienced that loss of appetite during stressful situations – when the thought of eating food just doesn’t cross the mind.
The Gut-Brain Axis and the Vagus Nerve
The GLP-1 produced in the intestines after a meal also plays a role in suppressing eating, likely through different circuits than those GLP-1-expressing neurons found in the brain stem. Researchers think that this involves the vagus nerve.[ref]
Vagus nerve interaction:
A 2026 study showed that the GLP-1 receptor is expressed in the nodose neurons, which are the sensory cells that transmit information from the internal organs to the brainstem.[ref]
GLP-1 Medications: Semaglutide, Tirzepatide, and Retatrutide
Given GLP-1’s powerful effects on appetite and glucose regulation, researchers developed synthetic medications that mimic its action.
The receptor for GLP-1 is the GLP-1 receptor (GLP1R gene, below in the genotype report section), a G-protein-coupled receptor. The GLP-1 receptor is a type of cell surface receptor that binds to GLP-1, triggering a signaling cascade that leads to various effects, including the stimulation of insulin secretion, the inhibition of gastric emptying, and the promotion of satiety.
History: In the early 2000s, GLP-1-based drugs (exenatide and liraglutide) were developed for the treatment of type 2 diabetes. Semaglutide was approved in 2017 and sold under the brand name Ozempic. These drugs are GLP-1 receptor agonists. An agonist is a type of drug or other agent that binds to a receptor on a cell and triggers a physiological response.
More recently, GLP-1 RA drugs have been approved for weight loss, cardiovascular disease, and chronic kidney disease. The following GLP-1 (glucagon-like peptide-1) receptor agonists are FDA-approved for weight loss:[ref]
| Brand Name | Generic Name | Type | Approved For |
|---|---|---|---|
| Ozempic | Semaglutide | GLP-1 RA | Type 2 diabetes |
| Wegovy | Semaglutide (higher dose) | GLP-1 RA | Weight loss |
| Mounjaro | Tirzepatide | GLP-1/GIP | Type 2 diabetes |
| Zepbound | Tirzepatide | GLP-1/GIP | Weight loss |
| Saxenda | Liraglutide | GLP-1 RA | Weight loss |
Retatrutide is a GLP-1/GIP/GCG triple agonist that is currently in trials for weight loss and diabetes, showing promise for weight loss without muscle loss (2026).
Side effects of GLP-1 RA medications:
While GLP-1 RAs offer significant benefits, it’s important to understand their potential drawbacks. They aren’t right for everyone, and the side effects can be significant. Please talk with your doctor about the risks and side effects before starting any GLP-1 medication.
Gastrointestinal adverse events:
The most common adverse effect is ‘gastrointestinal adverse events’. For example, in a semaglutide clinical trial in teens, gastrointestinal adverse events were reported in 62% of the group taking semaglutide, compared to 42% in the placebo group. Nausea, diarrhea, vomiting, and constipation commonly occur within the first month of starting.[ref][ref] Note that for many people, gastrointestinal side effects seem to be dose-related. Microdosing or starting with a lower dose may help to prevent gastrointestinal side effects.
Pancreatitis:
Case studies and a few of the clinical trials on GLP-1 RAs for diabetes have raised the possibility of pancreatitis being triggered by these drugs due to the potential growth in cells in the pancreas. As an example, one case study involving someone with a history of alcoholic pancreatitis tied an acute pancreatitis episode to starting semaglutide three months before. The FDA Adverse Event Reporting System shows a likely link between GLP-1 RAs (specifically liraglutide) and increased risk of pancreatitis. However, in a large study involving people with diabetes who had no comorbidities, GLP-1 RAs were not shown to increase the risk of developing pancreatitis at any time point up through 5 years of use.[ref][ref][ref][ref] The Cleveland Clinic now counsels that GLP-1 RA patients should be screened for pancreatitis risk factors, and a lower dose should be used to reduce the risk of pancreatitis.[ref]
Related article: Pancreatitis and Genetic Risk Factors
Gastroparesis:
Case reports tie semaglutide to a risk of gastroparesis (very slow stomach emptying). A large study that compared tirzepatide to semaglutide showed that in non-diabetic, overweight adults, the risk of gastroparesis was much higher in semaglutide recipients compared to tirzepatide. Out of over 17,000 patients on Tirzepatide, 10 reported gastroparesis. With the matched group on semaglutide, 28 reported gastroparesis.[ref][ref]
Diabetic retinopathy:
Two clinical trials in people with diabetes linked GLP-1 RA drugs to an increased risk of diabetic retinopathy, while other studies show that the drugs were not associated with the eye disease. A meta-analysis that combined data from systematic reviews and meta-analyses came to the conclusion that there was likely no increase in the risk of diabetic retinopathy from any of the diabetes drugs.[ref] However, this is still a side effect to be aware of and talk with your doctor about your individual risk.
Related article: Diabetes risk factors
Ischaemic optic neuropathy:
A 2026 study looked at FDA adverse event reporting from 2017 – 2024 for GLP-1 medications. The results showed that semaglutide use was linked to an increased relative risk of ischemic optic neuropathy, but tirzepetide was not. To put this into raw numbers, 84 cases of ischemic optic neuropathy were reported in people taking semaglutide over the 7 years. Monthly prescriptions of Ozempic during this time exceeded 2 million doses a month (not including Wegovy and other sources of semaglutide).[ref]
Understanding the mechanism behind these medications helps explain their effectiveness. Let’s dig into how and why these medications are effective.
How GLP-1 Receptor Agonists Cause Weight Loss
By binding to the GLP-1 receptor, GLP-1 RAs mimic the effects of having eaten and released GLP-1. In other words, you’ll feel full and won’t be driven to eat as much. The key is that GLP-1 RA medications are long-lasting receptor agonists that have an effect lasting much longer than naturally produced GLP-1. The medications resist being degraded by DPP-4, which is the enzyme that breaks down naturally produced GLP-1 within a few minutes. Semaglutide, when used as a subcutaneous injection, has a half-life of 5-6 days. Oral formulations have a shorter half-life.[ref]
In clinical trials, GLP-1 RAs improved lipid profiles, increased satiety, slowed gastric emptying, reduced inflammation, and had neuroprotective effects.[ref] The slowing of gastric emptying and reducing inflammation may play a role in weight loss, along with the decrease in appetite and eating less.
A combined effect that is bigger than just decreasing calories is thought to be at play when looking at the effects of activating the GLP-1 receptor.[ref]
In overweight adults aged 45+, a 4-year-long study using semaglutide for weight loss also prevented HbA1c from rising over time, which was seen in the placebo arm. The conclusion was that semaglutide for weight loss helps prevent overweight adults from progressing to diabetes.[ref]
Do Your Genes Determine How Well GLP-1s Work? (Pharmacogenomics)
The heritability of GLP-1 release is around 50%.[ref] Thus, while there is a fairly important genetic component, diet is also really important.
A recent study from the Cleveland Clinic showed that genetic variants also play a significant role in the response to GLP-1 RAs, like semaglutide, for weight loss. In the study, participants with a ‘responsive’ genetic score had an 82% increase in the likelihood of acheiving weight loss with a GLP-1 medication.[ref] Another study showed that GLP1 receptor variants are associated with greater weight loss on GLP-1 RA drugs.[ref]
Common genetic variants in the GLP1R (GLP-1 receptor) gene impact weight and type 2 diabetes risk. Variants in the DPP4 gene also affect GLP1 levels and diabetes risk. Your genotypes are covered in detail in the genotype report section below.
A 2026 study in mice also ties GLP1 receptor agonist effectiveness for weight loss to the body’s ability to use fatty acids for energy. Carnitine plays an essential role in the way that mitochondria use fats for fuel, and the study showed that mice deficient in a carnitine transporter, SLC25A45, didn’t lose weight as easily on a GLP-1 RA medication.[ref]
Related article: Carnitine genes
GLP-1 Beyond Weight Loss: Heart Disease, Alzheimer’s, Cancer, and Immunity
Recent studies show that the benefits of GLP-1 RA medications extend beyond weight loss.
GLP-1, Mast Cells, and Immune Response:
In addition to their role in pancreatic insulin secretion, GLP-1 receptors are found in certain types of immune cells, including T cells and macrophages.[ref] This is an interesting link between metabolic health and immune health, and microdosing GLP-1 medications is being looked at for preventing immune dysregulation in aging.
- Mast cell stabilizer (MCAS Connection):
GLP-1 receptors are also found on mast cells, and recent studies have shown that GLP-1 RA drugs prevent overactive mast cell degranulation. This may be of benefit for anyone with MCAS, and clinical trials are looking at the effectiveness of different doses.[ref][ref] (Related article: MCAS) - Immune system modulation:
The receptor for GLP-1 is found on the cell membrane of macrophages, regulatory T cells, and natural killer T cells. GLP-1 plays an immunomodulatory role. A GLP-1 receptor agonist medication may help patients with psoriasis.[ref]
Related article: T Cell Exhaustion
- Asthma symptoms decrease:
Asthma exacerbations also decreased in patients on GLP-1 receptor agonist medications.[ref] (Related article: Asthma genes)
Dementia and Alzheimer’s Prevention:
In animal studies, infusions of GLP-1 decrease amyloid-beta levels and prevent neuronal cell death.[ref] Dysregulation of glucose entry into the brain is one hallmark of Alzheimer’s disease, tying together insulin resistance, GLP-1, and dementia.[ref][ref] GLP-1 receptor agonist drugs, such as liraglutide, are being studied for Alzheimer’s disease.[ref]
Studies using data from diabetes patients showed a significant decrease in dementia for those on GLP-1s vs other diabetes medications. Some studies showed prevention benefits even in the absence of metabolic changes.[ref][ref] Studies are showing positive effects on cognitive function and possibly reduced (or delayed) dementia with GLP-1s. These effects are seen even outside of diabetes control.[ref]
Related article: APOE genotype and Alzheimer’s risk
Cardiovascular disease benefits:
A number of studies have shown that GLP-1 RAs provide benefits for reducing cardiovascular disease. The medications lower lipid levels and lower blood pressure in both diabetic and weight loss patients. Interestingly, the mechanism may be more than just weight loss. GLP-1 receptors are expressed in the heart muscle cells, immune system cells in the heart, and in the lining of blood vessels.[ref] GLP-1 RAs have been shown to help in heart failure and also to have beneficial effects on heart rhythm.[ref]
Related article: Cardiovascular disease genetic risk factors
Cancer Research:
Retatrutide, a GLP-1/GIP/GCG triple agonist, has recently been shown to reduce pancreatic tumor mass in animals. First, let me caution that this is just a mouse study, so it may not hold true in humans. A prior study had shown that retatrutide and semaglutide reduced pancreatic tumor mass in mice, along with weight loss. But the interesting thing about the new study is that the researchers used a low dose of retatrutide – one that was too low to cause weight loss. They found that even without causing weight loss, retatrutide had anti-tumor effects that were similar to the currently used (and incredibly expensive) immunotherapy.[ref]
A 5-year mortality study in colon cancer patients showed that GLP-1 RA use decreased mortality risk by 60% in obese patients.[ref] Animal studies may show the mechanism. Semaglutide has immunomodulatory and antitumor effects in a mouse model of breast cancer. Semaglutide promoted T cells to be able to respond more effectively to cancer.[ref]
More research is needed here, of course. Initial studies in rats caused concerns over GLP-1 RAs causing thyroid cancer, but human studies are less clear on whether it is a concern.[ref]
Decreased risk of substance abuse:
A large 2026 study using data from the VA showed that GLP-1 RA drugs reduce the risk of developing a substance addiction (drugs, alcohol). Moreover, for people already dealing with substance abuse, it decreased adverse events and the risk of death by 50%.[ref]
Phamacogenomics and GLP-1 RAs:
There’s an individual variability in treatment response to most medications, including GLP-1 RAs. Different genetic variants are associated with increased or decreased responses to GLP-1 RA drugs for diabetes or weight loss.
Researchers have found that differences in the GLP1RA gene, which encodes the GLP-1 receptor, influence how much weight someone is likely to lose on these medications. A recent genome-wide association study also identified the gene NBEA (neurobeachin) as likely contributing to differences in weight loss on GLP-1s. [ref]
Check out your genes below in the genotype report section:
Genotype Report: Check Your GLP-1 Genotype
Access this content:
An active subscription is required to access this content.
Lifehacks: Increase GLP-1 and Support Nutrition While on a GLP-1 RA
Let’s take a look at how to increase the effectiveness of GLP-1 RA drugs, natural alternatives to GLP-1 drugs, and dietary changes that impact GLP-1.
Strategies for weight loss with GLP-1s:
For those considering or currently using GLP-1 medications, here are several strategies that can enhance their effectiveness while minimizing side effects.
Works best with Exercise:
A randomized clinical trial found that GLP-1 RAs work best for weight loss when combined with exercise. The researchers compared exercise alone, exercise plus liraglutide, or liraglutide alone in people without diabetes. Exercise plus the GLP-1 RA worked best.[ref]
Works even at lower doses:
A 2025 study found that people who weren’t as consistent in taking daily doses or in taking the prescribed amount still had significant weight loss.[ref]
Dietary recommendations for reducing nausea:
Dietary recommendations for reducing nausea include avoiding fatty foods, eating well-cooked vegetables instead of raw ones, and including complex carbohydrates. Additionally, small, frequent meals are recommended, along with avoiding alcohol.[ref]
Benefits for CVD:
In a huge cardiovascular disease study, GLP-1 RAs were shown to be associated with a lower risk of heart attacks and strokes.[ref]
Nutritional considerations on a GLP-1 RA:
Nutrition researchers from Harvard recommend the following while on a GLP-1:[ref]
- Protein: Aim for 1 – 1.5g/kg of body weight in order to maintain muscle mass while on a GLP-1 RA.
- Energy: Smaller meals, but don’t skip meals. Keeping your energy up by not doing extended fasts.
- Avoid side effects: If you have nausea or gastrointestinal issues with a GLP-1, avoid high-fat foods and go with whole-grain toast. To avoid heartburn, eat smaller portions and eat your last meal three hours before bedtime.
Use your genes to find your susceptibility:
GLP-1s make it easy not to eat, which can end up causing nutritional deficiencies if you aren’t eating enough nutrient-dense whole foods. Use the vitamin and nutrients summary report to help you identify potential weak spots that are personal to your genes. For example, some people are more prone to folate deficiency and may need to supplement if not eating enough folate-rich foods.
Natural supplements that increase GLP-1:
Keep in mind that GLP-1 is quickly broken down in the body (within minutes). The effects of supplements that increase natural GLP-1 may not last long. Combining increased GLP-1 with a natural DPP4 inhibitor may help the effect to last a little longer. Theoretically, increasing GLP-1 before a meal may decrease appetite and the amount eaten.
Allulose:
A type of sugar that doesn’t raise blood sugar levels, allulose does trigger GLP-1 release.[ref] You can get allulose online or in health food stores as a sugar alternative.
Myricetin:
A natural flavonoid, myricetin, has been shown in animal studies to act as a GLP-1R agonist. Further studies are needed here, but it has the potential as a treatment for obesity and diabetes.[ref]
EGCG:
Found in green tea, EGCG has been shown in cell studies to increase GLP-1 secretion.[ref]
Yerba mate tea:
Animal studies show that Yerba mate induces GLP-1 secretion.[ref]
Increase bitterness:
The TAS2R38 gene, a bitter taste receptor, is active in the same cells in the gastrointestinal tract as glucagon-like peptide 1 cells. Recent research shows that bitter substances that activate TAS2R38 can also increase glucagon-like peptide 1 release.[ref]
Related article: Bitter Taste Receptors
Berberine: One bitter substance that activates TAS2R38 is berberine.[ref] Berberine is readily available as a supplement and also impacts blood glucose levels.
Related article: Berberine: Research Studies, Absorption, and Genetics
Curcumin:
Cell studies show that curcumin increases GLP-1 secretion in intestinal cells.[ref]
Related article: Curcumin Supplement Studies
Harmine:
Animal research shows that Peganum harmala, an herbal medicine plant, may help to protect the brain against Alzheimer’s disease. One impact of the plant (main constituents are harmine and harmaline) is that it increases GLP-1 in the hippocampus.[ref]
Lithium:
Lithium carbonate seems to suppress food intake (in some people) by activating GLP-1. Lithium carbonate is a prescription medication often prescribed for bipolar disorder.[ref]
Glutamine:
Glutamine is an amino acid that activates GLP-1 release.[ref] Foods that contain glutamine include eggs, beef, rice protein, pea protein, and tofu.[ref] Supplemental glutamine is available as a powder or in capsules. A study involving healthy, non-obese volunteers found that 6 g of glutamine increased GLP-1 secretion, but not enough to make much difference in glucose levels or appetite suppression.[ref]
Taurine:
Taurine is an important amino acid that is found in abundance in many seafoods and meats. A March 2025 study on mice found that taurine ‘enhanced GLP-1 secretion’. [ref]
Carnitine:
The study on mice showing that carnitine transport is essential for GLP-1 RA effectiveness indicates that low carnitine levels may impair weight loss.[ref] More studies are needed, but it may be that adding supplemental carnitine could help, especially if you have genetic variants related to lower carnitine levels.
Natural DPP4 inhibitors:
Research shows that several herbal supplements, including resveratrol, luteolin, and apigenin, inhibit DPP4. DPP4 is the enzyme that breaks down GLP-1, so by inhibiting DPP4, GLP-1 may hang around in the system longer. One study explained: “Out of all, the most potent DPP-IV inhibitors were found to be resveratrol, luteolin, apigenin and flavone having activity in nanomolar range”.[ref]
Related article: Resveratrol: Genetics and Bioavailability
Diets that increase GLP-1:[ref]
Olive oil:
Researchers have found that in addition to glucose, long-chain fatty acids also stimulate GLP-1 secretion in the small intestines. A study showed that people eating olive oil had a higher GLP-1 response than those who ate butter.
Plenty of protein:
Protein also stimulates the release of GLP-1. Specifically, egg whites, wheat protein, fish, and casein (dairy) cause the release of GLP-1.[ref]
Include fiber:
Fermentable fiber in the large intestines promotes the formation of short-chain fatty acids from the gut bacteria. Regularly eating fiber increases GLP-1 secretion due to the short-chain fatty acids produced in the microbiome.
Role of Circadian Rhythm in GLP-1:
The effectiveness of GLP-1 is also influenced by our body’s natural daily rhythms.
Your circadian rhythm is the 24-hour rhythm of your body’s functions. It controls when hormones are released, the production of enzymes at different times of the day, immune response during the day vs. night, sleep-wake timing, and much more.
A recent study examined the impact of sleep on people who have the GLP1R variant rs10305492 (the first gene in the genotype report). The study found that the combined effect of getting enough sleep plus the A allele was associated with a reduced risk of hyperglycemia and high HbA1c. [ref]
Circadian control of response to GLP-1:
Like many hormones, there is a circadian aspect to GLP-1. Research points to GLP-1 as having a role in entraining the circadian rhythm of insulin release in the pancreas. While GLP-1 will be released from intestinal cells upon consumption of food, the amount of insulin release that is triggered by GLP-1 varies due to the time of day.[ref]
Diet changes rhythm:
A ‘Western Diet’, high in fat and sugar, is used in research studies to induce obesity in animal models. Studies show that this type of diet actually alters the circadian rhythm of GLP-1 secretion, both in lab animals and in people with type 2 diabetes.[ref]
Does a decrease in natural GLP-1 secretion explain the obesity epidemic?
If you’re like me, you may be wondering what caused obesity to skyrocket over the past three decades – and whether GLP-1 has a role.
Often, the rise in obesity is explained as being due to people eating more and food being more appealing. However, that doesn’t quite fit with the availability of food over the century, the abundance of tasty cakes and pies, and the prior consumption of sugar (which has fallen since the 90s) and butter.
GLP-1 medications are known for quieting the ‘food noise’, meaning that they reduce the constant thoughts about eating, along with increasing satiety. At low doses, they take people back to a more normal food consumption pattern.
GLP-1 is produced in the cells lining the intestines, which makes gut health important. Multiple studies have tied changes in the gut microbiome to lower GLP-1 levels, but the mechanism isn’t always clearly defined.
A 2025 study in mice showed that prenatal glyphosate exposure at normal levels reshapes the gut microbiome. (Glyphosate is the herbicide in Roundup, and the use of glyphosate has risen dramatically over the last three decades. )
Specifically, the changes to the gut microbiome composition caused a reduction in the intestinal cells that produce mucin, which is the barrier that prevents microbes from causing inflammation in the gut. The changes resulted in a decrease in serum GLP-1 along with insulin resistance and metabolic dysfunction. The researchers suggest that changes in gut microbiome composition, particularly involving Akkermansia muciniphila and Parabacteroides distasonis, may explain the effects on GLP-1 and other gut-brain signaling molecules. Other studies have also linked glyphosate to metabolic dysfunction and changes to the gut microbiome, but this was the first study to also look at GLP-1 levels.[ref] [ref]
Related article: Glyphosate, genetics, metabolism
Another ubiquitous environmental exposure is BPA and BPS, which are chemicals used in plastics that act as endocrine disruptors. BPA and BPS exposure have been tied in numerous studies to metabolic dysfunction and obesity. It gets a little complicated, but essentially, BPA/BPS cause changes in a specific microRNA that controls GLP-1 levels. Cell studies show that BPA exposure directly causes a decrease in GLP-1 and insulin release through miR-338.[ref][ref]
Related article: BPA, BPS, Genetics, and Detoxification
Recap of your genes:
Access this content:
An active subscription is required to access this content.
FAQs:
Do genetics affect how well semaglutide works?
Yes, variants in the GLP1R gene (e.g., rs6923761) have been associated with differences in weight loss response to GLP-1 medications in clinical studies.
Why don’t GLP-1s work for me?
Individual response to GLP-1 medications varies. Genetic variants in the GLP-1 receptor, differences in gut microbiome composition, and carnitine metabolism may all play a role.
Is there a genetic test for GLP-1 response?
Research has identified specific gene variants associated with GLP-1 drug response, but pharmacogenomic testing for GLP-1 medications is not yet standard clinical practice. Raw genetic data from 23andMe or AncestryDNA can be checked for relevant variants.
Can you increase GLP-1 naturally?
Yes, several dietary strategies and supplements have been shown to boost GLP-1 production, including high-protein foods, olive oil, fermentable fiber, allulose, berberine, EGCG, and curcumin.
Does GLP-1 help with Alzheimer’s?
Research in animal models and population studies suggests GLP-1 receptor agonists may reduce dementia risk and improve cognitive function, but clinical trials are still ongoing.
Related Articles and Topics:
Intermittent Fasting: Benefits from changing Gene Expression
References:
Afrin, Lawrence B., et al. “Utility of Glucagon-like-Peptide-1-Receptor Agonists in Mast Cell Activation Syndrome.” The American Journal of the Medical Sciences, vol. 370, no. 4, Oct. 2025, pp. 377–82. DOI.org (Crossref), https://doi.org/10.1016/j.amjms.2025.07.006.
Brierley, Daniel I., et al. “Central and Peripheral GLP-1 Systems Independently Suppress Eating.” Nature Metabolism, vol. 3, no. 2, Feb. 2021, pp. 258–73. PubMed Central, https://doi.org/10.1038/s42255-021-00344-4.
—. “Central and Peripheral GLP-1 Systems Independently Suppress Eating.” Nature Metabolism, vol. 3, no. 2, Feb. 2021, pp. 258–73. PubMed Central, https://doi.org/10.1038/s42255-021-00344-4.
Cai, Miao, et al. “Glucagon-like Peptide-1 Receptor Agonists and Risk of Substance Use Disorders among US Veterans with Type 2 Diabetes: Cohort Study.” BMJ, vol. 392, Mar. 2026, p. e086886. DOI.org (Crossref), https://doi.org/10.1136/bmj-2025-086886.
Chedid, V., et al. “Allelic Variant in the Glucagon-like Peptide 1 Receptor Gene Associated with Greater Effect of Liraglutide and Exenatide on Gastric Emptying: A Pilot Pharmacogenetics Study.” Neurogastroenterology and Motility: The Official Journal of the European Gastrointestinal Motility Society, vol. 30, no. 7, July 2018, p. e13313. PubMed, https://doi.org/10.1111/nmo.13313.
de Graaf, Chris, et al. “Glucagon-Like Peptide-1 and Its Class B G Protein–Coupled Receptors: A Long March to Therapeutic Successes.” Pharmacological Reviews, vol. 68, no. 4, Oct. 2016, pp. 954–1013. PubMed Central, https://doi.org/10.1124/pr.115.011395.
—. “Glucagon-Like Peptide-1 and Its Class B G Protein–Coupled Receptors: A Long March to Therapeutic Successes.” Pharmacological Reviews, vol. 68, no. 4, Oct. 2016, pp. 954–1013. PubMed Central, https://doi.org/10.1124/pr.115.011395.
Diz-Chaves, Yolanda, et al. “Glucagon-Like Peptide-1 (GLP-1) in the Integration of Neural and Endocrine Responses to Stress.” Nutrients, vol. 12, no. 11, Oct. 2020, p. 3304. PubMed Central, https://doi.org/10.3390/nu12113304.
Eser, Hale Yapici, et al. “Association Between GLP-1 Receptor Gene Polymorphisms with Reward Learning, Anhedonia, and Depression Diagnosis.” Acta Neuropsychiatrica, vol. 32, no. 4, Aug. 2020, pp. 218–25. PubMed Central, https://doi.org/10.1017/neu.2020.14.
Femminella, Grazia Daniela, et al. “Evaluating the Effects of the Novel GLP-1 Analogue Liraglutide in Alzheimer’s Disease: Study Protocol for a Randomised Controlled Trial (ELAD Study).” Trials, vol. 20, no. 1, Apr. 2019, p. 191. PubMed, https://doi.org/10.1186/s13063-019-3259-x.
Foer, Dinah, et al. “Asthma Exacerbations in Patients with Type 2 Diabetes and Asthma on Glucagon-like Peptide-1 Receptor Agonists.” American Journal of Respiratory and Critical Care Medicine, vol. 203, no. 7, Apr. 2021, pp. 831–40. PubMed, https://doi.org/10.1164/rccm.202004-0993OC.
Gejl, Michael, et al. “Blood-Brain Glucose Transfer in Alzheimer’s Disease: Effect of GLP-1 Analog Treatment.” Scientific Reports, vol. 7, no. 1, Dec. 2017, p. 17490. PubMed, https://doi.org/10.1038/s41598-017-17718-y.
Geraedts, Maartje C. P., et al. “Direct Induction of CCK and GLP-1 Release from Murine Endocrine Cells by Intact Dietary Proteins.” Molecular Nutrition & Food Research, vol. 55, no. 3, Mar. 2011, pp. 476–84. PubMed, https://doi.org/10.1002/mnfr.201000142.
Gupta, Dharmendra Kumar, and Arunima Chaudhuri. “The Role of Glucagon-Like Peptide-1 Receptor Agonists in Cognitive Decline and Dementia Prevention: A Systematic Review and Semiquantitative Synthesis.” Journal of Mental Health and Human Behaviour, Aug. 2025. DOI.org (Crossref), https://doi.org/10.4103/jmhhb.jmhhb_71_25.
Greenfield, Jerry R., et al. “Oral Glutamine Increases Circulating GLP-1, Glucagon and Insulin Levels in Lean, Obese and Type 2 Diabetic Subjects.” The American Journal of Clinical Nutrition, vol. 89, no. 1, Jan. 2009, pp. 106–13. PubMed Central, https://doi.org/10.3945/ajcn.2008.26362.
Heo, Chan Uk, and Chang-Ik Choi. “Current Progress in Pharmacogenetics of Second-Line Antidiabetic Medications: Towards Precision Medicine for Type 2 Diabetes.” Journal of Clinical Medicine, vol. 8, no. 3, Mar. 2019, p. 393. PubMed Central, https://doi.org/10.3390/jcm8030393.
—. “Current Progress in Pharmacogenetics of Second-Line Antidiabetic Medications: Towards Precision Medicine for Type 2 Diabetes.” Journal of Clinical Medicine, vol. 8, no. 3, Mar. 2019, p. 393. PubMed Central, https://doi.org/10.3390/jcm8030393.
Hira, Tohru, et al. “Improvement of Glucose Tolerance by Food Factors Having Glucagon-Like Peptide-1 Releasing Activity.” International Journal of Molecular Sciences, vol. 22, no. 12, June 2021, p. 6623. PubMed Central, https://doi.org/10.3390/ijms22126623.
Hogan, A. E., et al. “Glucagon-like Peptide-1 (GLP-1) and the Regulation of Human Invariant Natural Killer T Cells: Lessons from Obesity, Diabetes and Psoriasis.” Diabetologia, vol. 54, no. 11, Nov. 2011, pp. 2745–54. PubMed, https://doi.org/10.1007/s00125-011-2232-3.
Holt, Marie K., et al. “Preproglucagon Neurons in the Nucleus of the Solitary Tract Are the Main Source of Brain GLP-1, Mediate Stress-Induced Hypophagia, and Limit Unusually Large Intakes of Food.” Diabetes, vol. 68, no. 1, Jan. 2019, pp. 21–33. PubMed Central, https://doi.org/10.2337/db18-0729.
Jarvela, Timothy S., et al. “Reduced Stability and PH-Dependent Activity of a Common Obesity-Linked PCSK1 Polymorphism, N221D.” Endocrinology, vol. 160, no. 11, Nov. 2019, pp. 2630–45. PubMed, https://doi.org/10.1210/en.2019-00418.
Jensterle, Mojca, et al. “Genetic Variability in GLP-1 Receptor Is Associated with Inter-Individual Differences in Weight Lowering Potential of Liraglutide in Obese Women with PCOS: A Pilot Study.” European Journal of Clinical Pharmacology, vol. 71, no. 7, July 2015, pp. 817–24. PubMed, https://doi.org/10.1007/s00228-015-1868-1.
—. “Genetic Variability in GLP-1 Receptor Is Associated with Inter-Individual Differences in Weight Lowering Potential of Liraglutide in Obese Women with PCOS: A Pilot Study.” European Journal of Clinical Pharmacology, vol. 71, no. 7, July 2015, pp. 817–24. PubMed, https://doi.org/10.1007/s00228-015-1868-1.
Kato, Masaki, et al. “Curcumin Improves Glucose Tolerance via Stimulation of Glucagon-like Peptide-1 Secretion.” Molecular Nutrition & Food Research, vol. 61, no. 3, Mar. 2017. PubMed, https://doi.org/10.1002/mnfr.201600471.
Kulanuwat, Sirikul, et al. “Effects of PCSK1 Genetic Variants on Obesity among Thai Children and Their Family Members: In Relation to Health Risk, and Biochemical and Anthropometric Parameters.” The Southeast Asian Journal of Tropical Medicine and Public Health, vol. 45, no. 1, Jan. 2014, pp. 214–25.
Lakhani, Moiz, et al. “Ischemic Optic Neuropathy with Semaglutide: Global Observational Analysis of Sex- and Formulation-Specific Risk.” The British Journal of Ophthalmology, Mar. 2026, p. bjo-2025-328483. PubMed, https://doi.org/10.1136/bjo-2025-328483.
Löffler, Dennis, et al. “Functional and Clinical Relevance of Novel and Known PCSK1 Variants for Childhood Obesity and Glucose Metabolism.” Molecular Metabolism, vol. 6, no. 3, Mar. 2017, pp. 295–305. PubMed, https://doi.org/10.1016/j.molmet.2016.12.002.
Martchenko, Alexandre, and Patricia Lee Brubaker. “Effects of Obesogenic Feeding and Free Fatty Acids on Circadian Secretion of Metabolic Hormones: Implications for the Development of Type 2 Diabetes.” Cells, vol. 10, no. 9, Sept. 2021, p. 2297. www.mdpi.com, https://doi.org/10.3390/cells10092297.
Mariam‐Smith, Arshiya, et al. “Neurobeachin ( NBEA ) Is a Novel Gene Associated with GLP ‐1 Receptor Agonist Associated Weight Loss.” Diabetes, Obesity and Metabolism, vol. 27, no. 10, Oct. 2025, pp. 5632–42. DOI.org (Crossref), https://doi.org/10.1111/dom.16612.
Mehrtash, Farhad, et al. “I Am Taking a GLP-1 Weight-Loss Medication—What Should I Know?” JAMA Internal Medicine, vol. 185, no. 9, Sept. 2025, p. 1180. DOI.org (Crossref), https://doi.org/10.1001/jamainternmed.2025.1133.
Merchant, Warda, et al. “Glucagon‐Like Peptide‐1 Targets in the Human Nodose Ganglion.” Journal of Comparative Neurology, vol. 534, no. 2, Feb. 2026, p. e70135. DOI.org (Crossref), https://doi.org/10.1002/cne.70135.
—. “Effects of Obesogenic Feeding and Free Fatty Acids on Circadian Secretion of Metabolic Hormones: Implications for the Development of Type 2 Diabetes.” Cells, vol. 10, no. 9, Sept. 2021, p. 2297. www.mdpi.com, https://doi.org/10.3390/cells10092297.
Mbikay, Majambu, et al. “Effects of Rs6234/Rs6235 and Rs6232/Rs6234/Rs6235 PCSK1 Single-Nucleotide Polymorphism Clusters on Proprotein Convertase 1/3 Biosynthesis and Activity.” Molecular Genetics and Metabolism, vol. 104, no. 4, Dec. 2011, pp. 682–87. PubMed, https://doi.org/10.1016/j.ymgme.2011.09.027.
—. “Effects of Rs6234/Rs6235 and Rs6232/Rs6234/Rs6235 PCSK1 Single-Nucleotide Polymorphism Clusters on Proprotein Convertase 1/3 Biosynthesis and Activity.” Molecular Genetics and Metabolism, vol. 104, no. 4, Dec. 2011, pp. 682–87. PubMed, https://doi.org/10.1016/j.ymgme.2011.09.027.
Meek, Claire L., et al. “The Effect of Encapsulated Glutamine on Gut Peptide Secretion in Human Volunteers.” Peptides, vol. 77, Mar. 2016, pp. 38–46. PubMed, https://doi.org/10.1016/j.peptides.2015.10.008.
Müller, T. D., et al. “Glucagon-like Peptide 1 (GLP-1).” Molecular Metabolism, vol. 30, Sept. 2019, pp. 72–130. PubMed Central, https://doi.org/10.1016/j.molmet.2019.09.010.
—. “Glucagon-like Peptide 1 (GLP-1).” Molecular Metabolism, vol. 30, Sept. 2019, pp. 72–130. PubMed Central, https://doi.org/10.1016/j.molmet.2019.09.010.
Perry, TracyAnn, et al. “Glucagon-like Peptide-1 Decreases Endogenous Amyloid-Beta Peptide (Abeta) Levels and Protects Hippocampal Neurons from Death Induced by Abeta and Iron.” Journal of Neuroscience Research, vol. 72, no. 5, June 2003, pp. 603–12. PubMed, https://doi.org/10.1002/jnr.10611.
Pham, Hung, et al. “A Bitter Pill for Type 2 Diabetes? The Activation of Bitter Taste Receptor TAS2R38 Can Stimulate GLP-1 Release from Enteroendocrine L-Cells.” Biochemical and Biophysical Research Communications, vol. 475, no. 3, July 2016, pp. 295–300. PubMed Central, https://doi.org/10.1016/j.bbrc.2016.04.149.
Qi, Qibin, et al. “Association of PCSK1 Rs6234 with Obesity and Related Traits in a Chinese Han Population.” PloS One, vol. 5, no. 5, May 2010, p. e10590. PubMed, https://doi.org/10.1371/journal.pone.0010590.
Saleh, Rofida A., et al. “Peganum Harmala Enhanced GLP-1 and Restored Insulin Signaling to Alleviate AlCl3-Induced Alzheimer-like Pathology Model.” Scientific Reports, vol. 11, no. 1, June 2021, p. 12040. PubMed, https://doi.org/10.1038/s41598-021-90545-4.
Sheikh, Haroon I., et al. “Glucagon-Like Peptide-1 Receptor Gene Polymorphism (Leu260Phe) Is Associated With Morning Cortisol in Preschoolers.” Progress in Neuro-Psychopharmacology & Biological Psychiatry, vol. 34, no. 6, Aug. 2010, pp. 980–83. PubMed Central, https://doi.org/10.1016/j.pnpbp.2010.05.007.
Singla, Rajeev K., et al. “Natural Products: Potential Source of DPP-IV Inhibitors.” Current Protein & Peptide Science, vol. 20, no. 12, 2019, pp. 1218–25. PubMed, https://doi.org/10.2174/1389203720666190502154129.
Torekov, S. S., et al. “Homozygous Carriers of the G Allele of Rs4664447 of the Glucagon Gene (GCG) Are Characterised by Decreased Fasting and Stimulated Levels of Insulin, Glucagon and Glucagon-like Peptide (GLP)-1.” Diabetologia, vol. 54, no. 11, Nov. 2011, pp. 2820–31. PubMed, https://doi.org/10.1007/s00125-011-2265-7.
Vrang, Niels, et al. “Gastric Distension Induces C-Fos in Medullary GLP-1/2-Containing Neurons.” American Journal of Physiology. Regulatory, Integrative and Comparative Physiology, vol. 285, no. 2, Aug. 2003, pp. R470-478. PubMed, https://doi.org/10.1152/ajpregu.00732.2002.
Wessel, Jennifer, et al. “Low-Frequency and Rare Exome Chip Variants Associate with Fasting Glucose and Type 2 Diabetes Susceptibility.” Nature Communications, vol. 6, Jan. 2015, p. 5897. PubMed Central, https://doi.org/10.1038/ncomms6897.
Yildirim Simsir, Ilgin, et al. “Glucagon like Peptide-1 (GLP-1) Likes Alzheimer’s Disease.” Diabetes & Metabolic Syndrome, vol. 12, no. 3, May 2018, pp. 469–75. PubMed, https://doi.org/10.1016/j.dsx.2018.03.002.
—. “Glucagon like Peptide-1 (GLP-1) Likes Alzheimer’s Disease.” Diabetes & Metabolic Syndrome, vol. 12, no. 3, May 2018, pp. 469–75. PubMed, https://doi.org/10.1016/j.dsx.2018.03.002.
Yue, Xiao, et al. “Berberine Activates Bitter Taste Responses of Enteroendocrine STC-1 Cells.” Molecular and Cellular Biochemistry, vol. 447, no. 1–2, Oct. 2018, pp. 21–32. PubMed, https://doi.org/10.1007/s11010-018-3290-3.